
Neonatal Hemodynamics and Cardiovascular Medicine
Session: Neonatal Hemodynamics and Cardiovascular Medicine 3
.jpeg.jpg "John Wren, MD PhD photo")
John Wren, MD PhD
Clinical Assistant Professor
University of Iowa Stead Family Children's Hospital
Iowa City, Iowa, United States
.png) (A) Sankey diagram depicting individual hemodynamic phenotypes and their transitions over time and their relation to survival to discharge. For the first two timepoints, the first targeted neonatal echocardiogram (TNE) <24 hours and the first TNE between 24-72 hours was included. The last TNE prior to operative diaphragm repair and the first TNE post-repair was included for the last two time points. (B-D) Algorithm of phenotype classification employed at each timepoint based on the applicable TNE. Predominant ventricular systolic dysfunction was determined via a comparison of left (LV) and right ventricular (RV) echocardiography measures including ejection fraction by Simpon's biplane, LV s' and tricuspid annular plane systolic excursion (TAPSE), RV s', and RV fractional area change, respectively. Patent ductus arteriosus (PDA) shunt direction was determined quantitatively via percent left-to-right (LR) by velocity time integral (VTI). Atrial shunt direction was subjectively categorized. Flow reversal in the descending aorta, a recognized marker of ductal steal/pulmonary over-circulation in preterm neonates, was only considered present if it was present throughout diastole (holodiastolic). PH, pulmonary hypertension; Pr LR, predominant left-to-right; bid, bidirectional; Pr RL, predominant right-to-left; RL, right-to-left; RVSp, estimated right ventricular systolic pressure (+ right atrial pressure); sEI, systolic eccentricity index; iNO, inhaled nitric oxide; PGE, prostaglandin E infusion; DAo, descending aorta.
(A) Sankey diagram depicting individual hemodynamic phenotypes and their transitions over time and their relation to survival to discharge. For the first two timepoints, the first targeted neonatal echocardiogram (TNE) <24 hours and the first TNE between 24-72 hours was included. The last TNE prior to operative diaphragm repair and the first TNE post-repair was included for the last two time points. (B-D) Algorithm of phenotype classification employed at each timepoint based on the applicable TNE. Predominant ventricular systolic dysfunction was determined via a comparison of left (LV) and right ventricular (RV) echocardiography measures including ejection fraction by Simpon's biplane, LV s' and tricuspid annular plane systolic excursion (TAPSE), RV s', and RV fractional area change, respectively. Patent ductus arteriosus (PDA) shunt direction was determined quantitatively via percent left-to-right (LR) by velocity time integral (VTI). Atrial shunt direction was subjectively categorized. Flow reversal in the descending aorta, a recognized marker of ductal steal/pulmonary over-circulation in preterm neonates, was only considered present if it was present throughout diastole (holodiastolic). PH, pulmonary hypertension; Pr LR, predominant left-to-right; bid, bidirectional; Pr RL, predominant right-to-left; RL, right-to-left; RVSp, estimated right ventricular systolic pressure (+ right atrial pressure); sEI, systolic eccentricity index; iNO, inhaled nitric oxide; PGE, prostaglandin E infusion; DAo, descending aorta. .png) Hemodynamic phenotypes were delineated via a standardized algorithm seen in Figure 1. Data are expressed as the mean (standard deviation) except where indicated. Blank/shaded columns indicate no TNEs fit into that phenotype at that time point. Statistical analysis via Kruskal-Willis for the <24 hour, 24-72 hours, and pre-operative time point and Mann-Whitney for the post-operative time point was utilized for continuous variables and Fisher's exact test was utilized for categorical variables. P < 0.05 was considered statistically significant. a,b denote statistical significance between matched subgroups by Dunn's multiple comparisons test. PH, pulmonary hypertension, TNE, targeted neonatal echocardiography; VIS, vasoactive inotrope score; iNO, inhaled nitric oxide; PGE, prostaglandin infusion; PDA, patent ductus arteriosus; ECLS, extracorporeal life support.
Hemodynamic phenotypes were delineated via a standardized algorithm seen in Figure 1. Data are expressed as the mean (standard deviation) except where indicated. Blank/shaded columns indicate no TNEs fit into that phenotype at that time point. Statistical analysis via Kruskal-Willis for the <24 hour, 24-72 hours, and pre-operative time point and Mann-Whitney for the post-operative time point was utilized for continuous variables and Fisher's exact test was utilized for categorical variables. P < 0.05 was considered statistically significant. a,b denote statistical significance between matched subgroups by Dunn's multiple comparisons test. PH, pulmonary hypertension, TNE, targeted neonatal echocardiography; VIS, vasoactive inotrope score; iNO, inhaled nitric oxide; PGE, prostaglandin infusion; PDA, patent ductus arteriosus; ECLS, extracorporeal life support.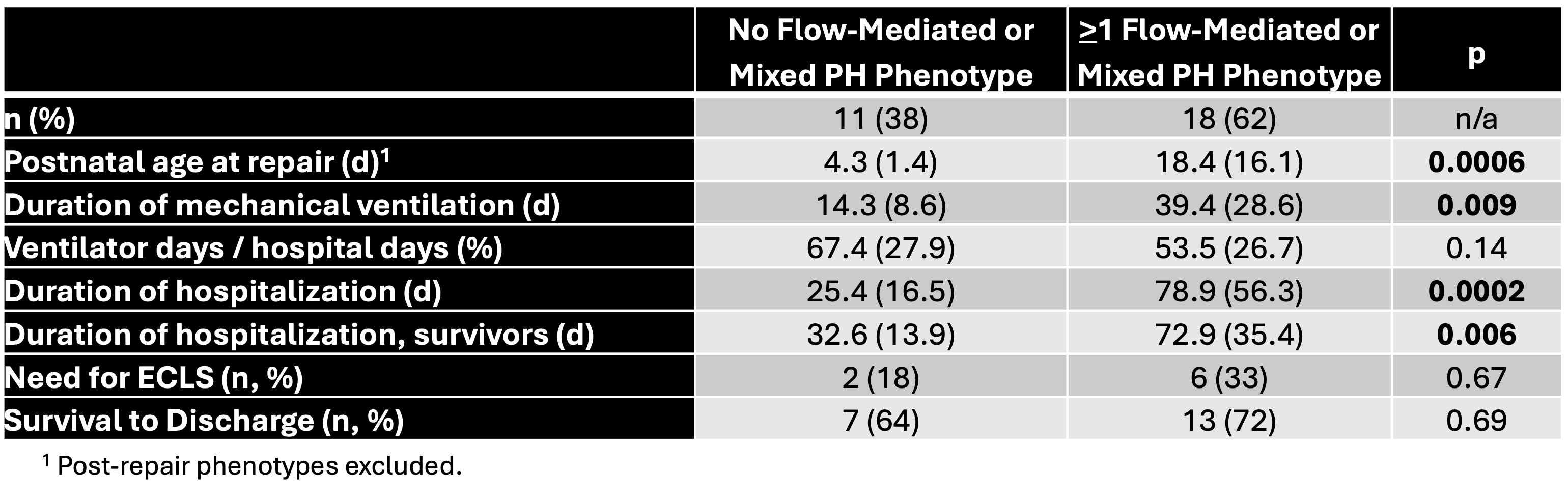 Hemodynamic phenotypes were delineated via a standardized algorithm seen in Figure 1. Data are presented as the mean (standard deviation) unless otherwise indicated. PH, pulmonary hypertension; ECLS, extracorporeal life support. Statistical analysis via Mann-Whitney test. P < 0.05 considered statistically significant.
Hemodynamic phenotypes were delineated via a standardized algorithm seen in Figure 1. Data are presented as the mean (standard deviation) unless otherwise indicated. PH, pulmonary hypertension; ECLS, extracorporeal life support. Statistical analysis via Mann-Whitney test. P < 0.05 considered statistically significant.