504 - Redefining risk: The impact of early onset sepsis definitions on incidence and 14-Day mortality in preterm infants — a population-based study in Canada, 2010–2023
Sunday, April 26, 2026
9:30am - 11:30am ET
Publication Number: 3485.504
Qi Zhou, The Hospital for Sick Children, Toronto, ON, Canada; Shoo Lee, University of Toronto Temerty Faculty of Medicine, Edmonton, AB, Canada; Vann Chau, The Hospital for Sick Children, Toronto, ON, Canada; Marc Beltempo, McGill University, Montreal, PQ, Canada; Shikha Gupta-Bhatnagar, McMaster Children's Hospital, Hamilton, ON, Canada; Paloma Costa, The Moncton Hospital, Moncton, NB, Canada; Chelsea Ruth, Max Rady College of Medicine, Rady Faculty of Health Sciences, University of Manitoba, Winnipeg, MB, Canada; Yi-Chen Su, mount sinai hospital, Toronto, ON, Canada; Joseph Ting, University of Alberta, Edmonton, AB, Canada
Associate Professor University of Alberta Edmonton, Alberta, Canada
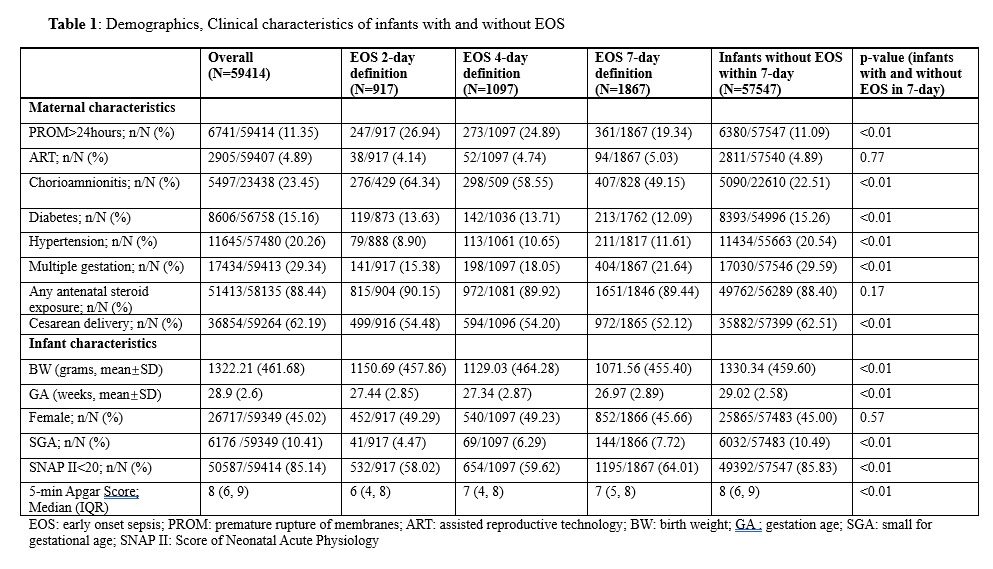
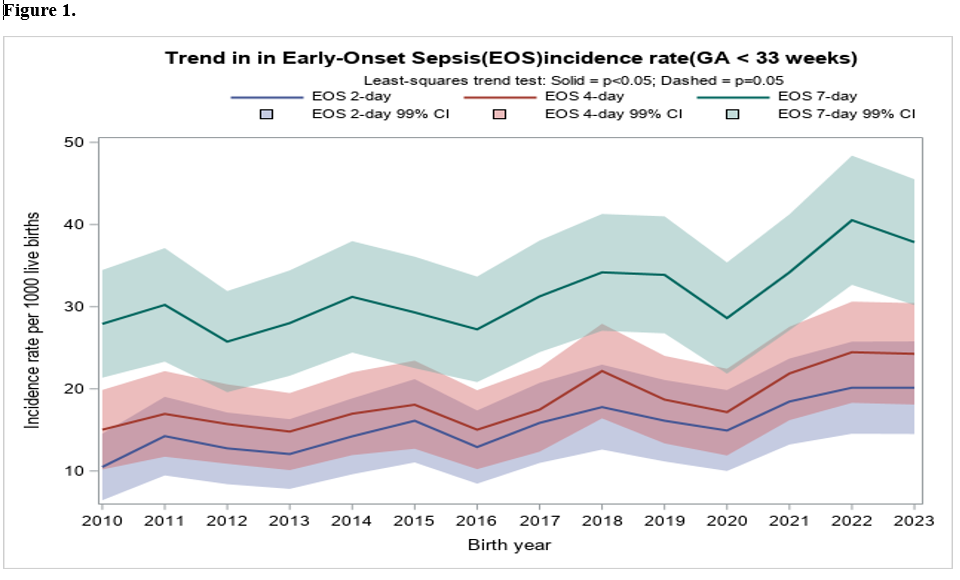
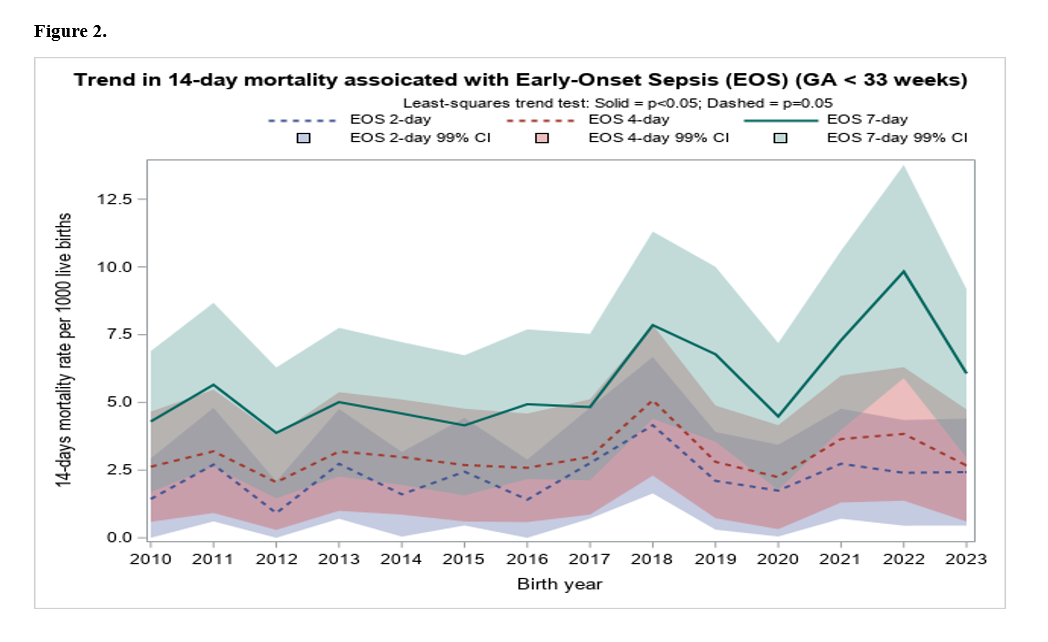
Background: Early-onset sepsis (EOS) remains an important cause of neonatal mortality and morbidity among very preterm infants. The definition of EOS varies widely across the literature, ranging from infections occurring within the first 48 hours to 7 days after birth which complicates surveillance and comparative research. Objective: Our objective was to evaluate how differing definitions of EOS affect reported incidence and mortality in preterm infants, and to assess temporal trends based on these varying definitions. Design/Methods: We conducted a retrospective cohort study using data from the Canadian Neonatal Network (CNN) database, which included infants born at < 33 weeks gestational age (GA) and admitted to 32 tertiary neonatal intensive care units (NICUs) across Canada between 2010 and 2023. We compared demographic and clinical characteristics, and outcomes among infants without EOS, and those meeting three definitions of EOS based on timing of diagnoses: within 2, 4 and 7 calendar days of birth. EOS-related mortality was defined as death occurring within 14 days of EOS diagnosis. We analyzed trends in EOS incidence and identified the organisms cultured across the study period. Results: We identified 59,761 infants eligible for this study, excluding 347 due to incomplete data or moribund status on admission. Compared to infants without EOS, those meeting EOS definitions were more likely to be associated with prolonged rupture of membranes, clinical chorioamnionitis, antenatal corticosteroid exposure, lower gestational age, lower 5 minute Apgar scores, and higher SNAP II scores, and less likely to have maternal diabetes and hypertension, multiple gestation or caesarean delivery (Table 1). EOS incidence increased with broader definitions: 15.4, 18.4, and 31.4 per 1,000 live births for the 2, 4, and 7 day definitions, respectively. The 14-day mortality rose from 2.2 to 3.0 and 5.6 per 1,000 live births across the same definitions. All three EOS definitions demonstrated an increasing trend in incidence over time (Figure 1), while the 7-day definition also showed a secular rise in 14 day mortality (Figure 2) from 2010 to 2023. In all definitions, E.coli (5.41-8.69 per 1000 live births) was the most frequently isolated pathogen, followed by GBS (7.28-13.96 per 1000 live births), and other organisms (Streptococcus viridans, Klebsiella species, and Enterococcus species).
Conclusion(s): There has been a consistent increase in EOS over time. The choice of definition significantly influences the reported incidence and 14-day mortality, underscoring the need for standardized criteria in surveillance and clinical practice.
Demographics, Clinical characteristics of infants with and without EOS
Trend in Early-Onset Sepsis incidence rate (GA <33weeks)
Trend in 14-day mortality associated with Early-Onset Sepsis (GA <33weeks)

.jpg "Joseph Ting, MD, MPH photo")