TOP 54 - Differentiating Ventilator Associated Pulmonary Infection from Tracheal Bacterial Colonization in VLBW Newborns
Friday, April 24, 2026
5:30pm - 8:00pm ET
Publication Number: 1813.TOP 54
Claire Gallibois, MedStar Georgetown University Hospital, Washington, DC, United States; Raymond K.. Brown-Riley, Medstar Georgetown University Hospital, Washington, DC 20007, DC, United States; Kabir Abubakar, Georgetown University School of Medicine, Washington, DC, United States; Arash R.. Zandieh, Georgetown University School of Medicine, Washington, DC, United States; Jayashree Ramasethu, MedStar Georgetown University Hospital, Washington, DC, United States
Neonatology Fellow MedStar Georgetown University Hospital, United States
Background: Ventilator associated pulmonary infection (VAPI) is a hospital acquired lower airway infection in intubated patients associated with significant morbidity and mortality. In neonatal intensive care units (NICUs), the wide range of 2.7 - 37.2 episodes of VAPI per 1000 ventilator days reveals the challenges in correctly diagnosing VAPI. The CDC National Healthcare Safety Network criteria for diagnosing VAPIs in infants < 1 year old are not suitable for very low birth weight (VLBW, ≤1500g) infants who are at highest risk and where evolving chronic lung disease may obfuscate diagnosis. Differentiating VAPI from tracheal bacterial colonization (TBC) is difficult and important for treatment decisions and antibiotic stewardship. Tracheal cultures are used more often than bronchoalveolar lavage for diagnosis in the NICU. Objective: To differentiate VAPI from TBC in VLBW infants by scoring several variables to determine the importance of each individually and in combination to arrive at a diagnosis. Design/Methods: This retrospective IRB approved chart review includes VLBW infants admitted to a level 4 NICU from 01/2018 to 12/2024 with tracheal cultures performed while on mechanical ventilation for at least 48 hours. Data included patient demographics, clinical signs, tracheal gram stain/cultures, quality/ quantity of tracheal aspirate, ventilator duration, changes in mean airway pressure (MAP), fraction of inspired oxygen (FiO2) 72 hours before and 3 to 7 days after tracheal cultures, respiratory/cardiac/infectious comorbidities, complete blood counts, treatment and outcomes. Xrays prior to, on day of tracheal culture (± 1 day) and 2- 5 days after tracheal culture were selected by a neonatologist (JR), and are being reviewed and graded using a validated grading system by a pediatric radiologist (AZ) and a neonatologist (KA) - all three are blinded to the results of the tracheal culture. These variables are being scored and weighted to determine VAPI diagnosis versus TBC. Data analysis including correlation analysis and multinominal logistic regression will be completed by January.
Preliminary
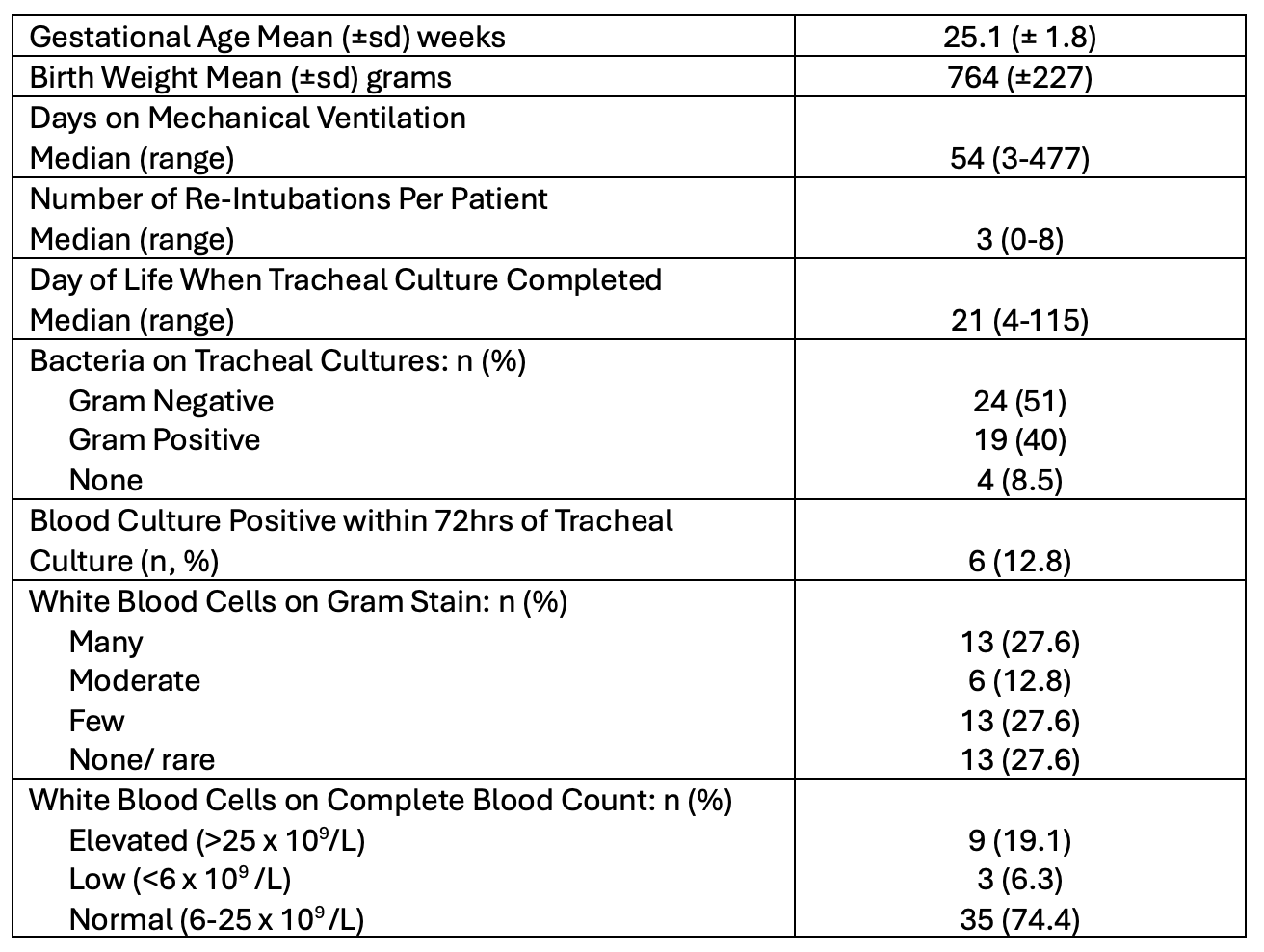
Results: Table 1 shows preliminary data on 47 VLBW patients with tracheal cultures. Twenty-five (57%) of infants with a positive culture had 10% or more increase in FiO2 in the 72hrs pre -culture, and but this improved in 25 (53%) of infants by 7 days post culture. Ventilator MAPs increased by 2 mm Hg or more in 22 (47%) infants prior to the culture and this improved in 18 (38%) of infants 7 days post -culture.

 photo")