TOP 35 - Predicting Extubation Success Using Lung Ultrasound in Chronically Ventilated Premature Infants exposed to Postnatal Dexamethasone
Friday, April 24, 2026
5:30pm - 8:00pm ET
Publication Number: 1795.TOP 35
Hemanthi Durga Veligaram, University of Kentucky College of Medicine, Richmond, KY, United States; Ravi Bhavsar, University of Kentucky College of Medicine, Lexington, KY, United States; Ianna Blanchard, University of Kentucky Children's Hospital, Lexington, KY, United States; Rupin Kumar, University of Kentucky College of Medicine, Lexington, KY, United States; Mina Hanna, Kentucky Children's Hospital, Lexington, KY, United States; Prasad Bhandary, University of Kentucky, Lexington, KY, United States
Fellow Physician University of Kentucky College of Medicine Richmond, Kentucky, United States
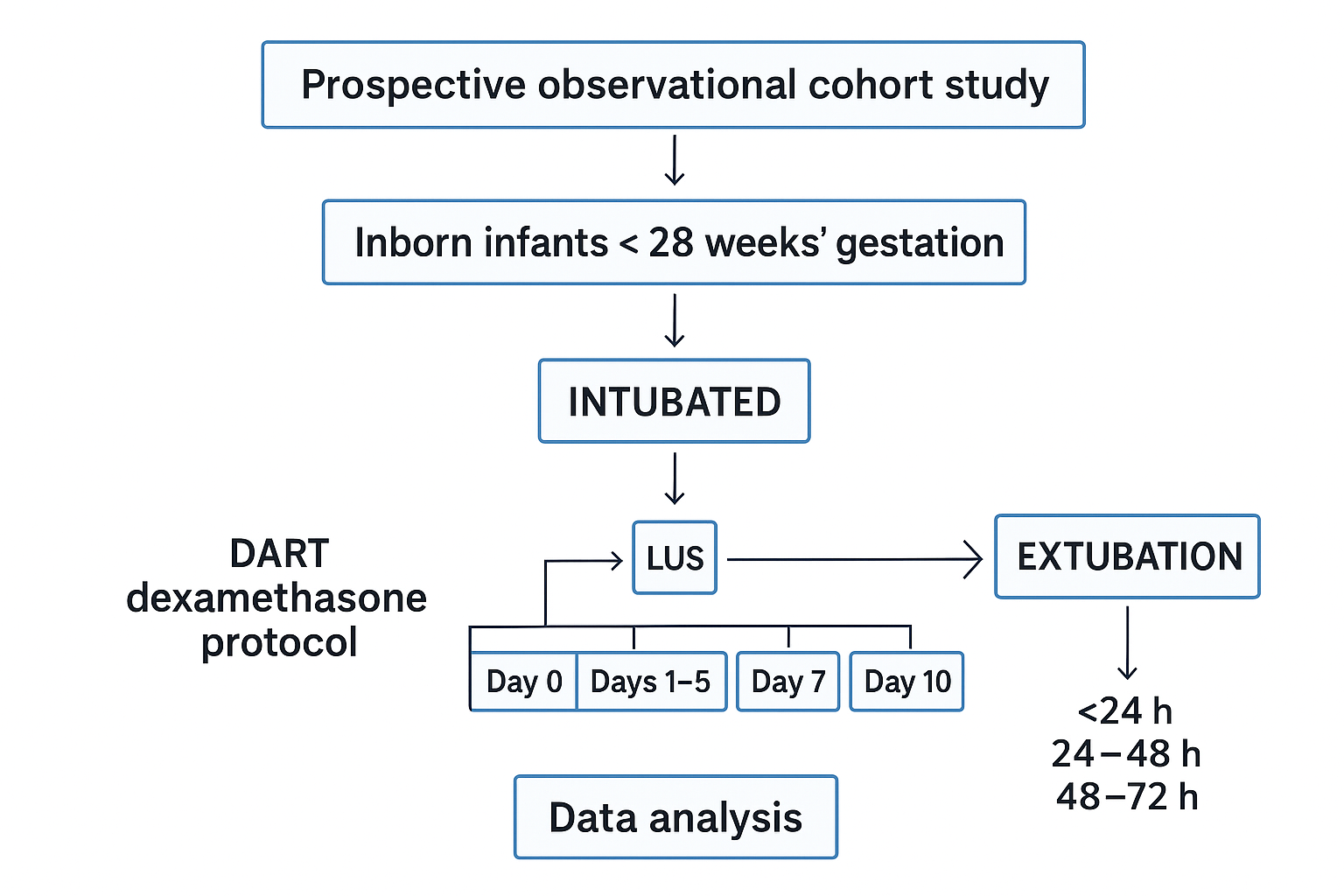
Background: Lung ultrasonography (LUS) is a rapid, radiation‑free bedside imaging tool used to assess a variety of lung pathologies, including bronchopulmonary dysplasia (BPD). Systemic corticosteroids have been shown to reduce inflammation and promote extubation, but timing and dose are critical. The 10‑day low‑dose DART dexamethasone taper improves extubation rates yet carries risks of adverse neurodevelopmental outcomes. LUS scores (LUSc) are validated in RDS to track lung aeration and correlate with FiO2 requirements. This study uses serial LUSc to objectively measure pulmonary response to low‑dose dexamethasone in mechanically ventilated preterm infants and identify predictors of successful extubation. Objective: 1. To objectively monitor response to postnatal low‑dose dexamethasone in intubated preterm infants using serial LUSC and evaluate correlations with ventilator mean airway pressure and oxygenation indices. 2. To identify baseline clinical and demographic variables associated with successful extubation following the dexamethasone course. Design/Methods: This is a prospective, observational cohort study of inborn infants < 28 weeks' gestation who are intubated and receiving the dexamethasone protocol to facilitate extubation. Infants with major congenital anomalies or known syndromes are excluded. Baseline maternal and neonatal demographics and clinical data will be collected. LUSc will follow the validated system by DeLuca et al. LUS examinations will be performed using MindRay TE7 and Sonosite X‑porte machines with 22 MHz probes and recorded in a HIPAA‑compliant institutional image repository. Scheduled LUS timepoints are Day 0 (initiation), Days 1-5, Day 7, and Day 10 of the dexamethasone course. For infants extubated during the study period, LUS will be obtained at < 24 h, 24-48 h, and 48-72 h post‑extubation. Images will be de-identified and independently reviewed by two blinded experts; inter‑observer agreements will be calculated. Ventilator parameters, mean airway pressure, and oxygenation indices) will be extracted from the electronic health record. Spearman's correlation will assess relationships between LUSc and ventilatory/oxygenation measures over time. Logistic regression will identify baseline predictors of successful versus unsuccessful extubation. Descriptive statistics will summarize cohort characteristics. Our study is IRB‑approved, and 34 subjects have been enrolled to date. Data analysis will be completed before January 31, 2026.