Session: Health Equity/Social Determinants of Health 3
206 - Trends in Health Care Disparities Between U.S.-Born and Immigrant Children Across States, 2016–2023
Friday, April 24, 2026
5:30pm - 8:00pm ET
Publication Number: 1195.206
Aditi Doiphode, Icahn School of Medicine at Mount Sinai, New York, NY, United States; Megan E. Paul, Stanford University School of Medicine, Sunnyvale, CA, United States; Laurel E. Wong, Icahn School of Medicine at Mount Sinai, New York, NY, United States; Brian A. Coakley, Seattle Children's Hospital -- University of Washington, Seattle, WA, United States
Medical Student Icahn School of Medicine at Mount Sinai New York, New York, United States
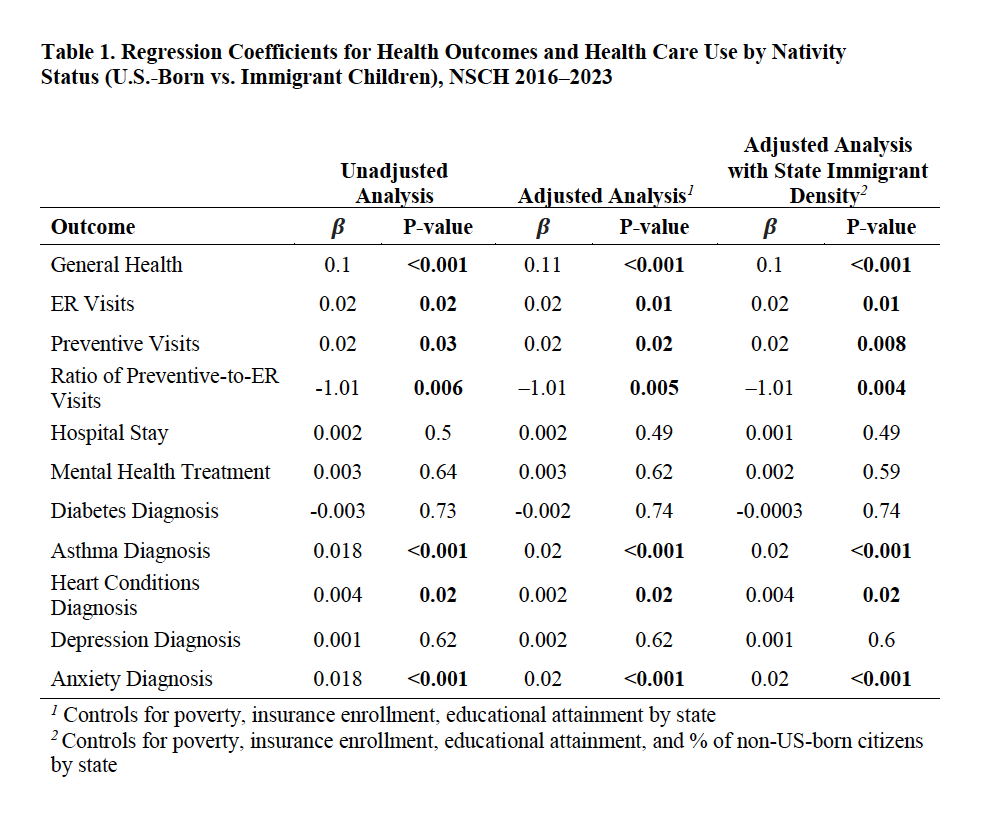
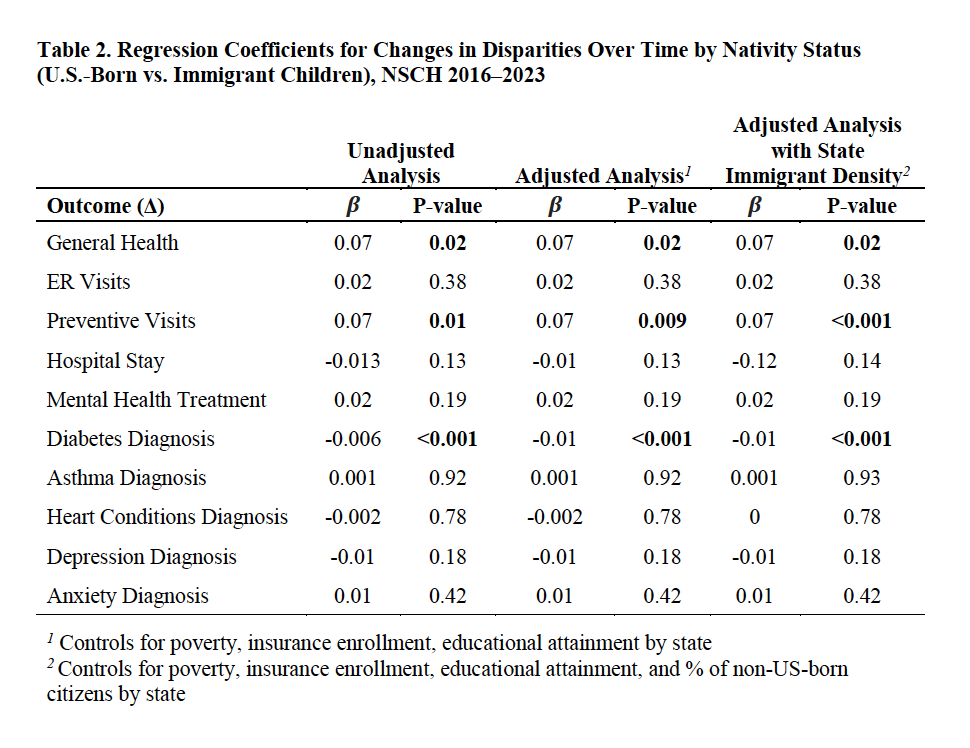
Background: In the United States (US), immigrant children face many unique social and economic challenges, including difficulty accessing proper healthcare. While health inequities among immigrant children have been previously documented, prior studies have not accounted for state-level factors known to shape pediatric health outcomes. Objective: This study aims to assess healthcare disparities between US-born and non-US-born children, while adjusting for state-level factors and examining trends over time. Design/Methods: National Survey of Children's Health data from 2016-2023 was compared among U.S-born and immigrant children using multivariable regression. Outcome variables included caregiver-reported general health, preventive visits, emergency room (ER) visits, hospital stays, mental health treatment, and diagnosis of specified medical comorbidities (heart disease, asthma, diabetes, anxiety or depression). Three regression models were analyzed (1) unadjusted, (2) adjusted for state-level poverty, insurance coverage, and parental education, and (3) adjusted for state immigrant population density. Results: Non-immigrant status was associated with better caregiver-reported health quality (β = +0.10, p< 0.001), more preventive (β = +0.02, p< 0.01) and ER visits (β = +0.02, p< 0.05), as well as higher rates of asthma (β = +0.02, p< 0.001), anxiety (β = +0.02, p< 0.001), and heart conditions (β = +0.004, p< 0.05) diagnoses. While immigrant status was associated with lower utilization of both preventive and ER care, a significantly higher preventive-to-ER visit ratio was observed (β = -1.01, p< 0.01). From 2016 to 2023, non-immigrant status was also associated with greater increases in preventive visits (Δβ = +0.07, p< 0.001) and better general health over time (Δβ = +0.07, p< 0.05). Overall prevalence of diabetes between U.S.-born and immigrant children was not significantly different, but the rate of diabetes diagnoses rose faster among immigrant children (Δβ = -0.01, p< 0.001). Results were consistent across all models, indicating disparities persist after adjustment.
Conclusion(s): Health disparities between US-born and immigrant children are apparent and worsening. US-born children are more commonly diagnosed with medical comorbidities, which may represent greater overall healthcare access. While immigrant children access less care overall, they tend to use more preventive care than emergent care. Efforts to eliminate health disparities among immigrant children should focus on expanding healthcare access.
Table 1. Regression Coefficients for Health Outcomes and Health Care Use by Nativity Status (U.S.-Born vs. Immigrant Children), NSCH 2016-2023
Table 2. Regression Coefficients for Changes in Disparities Over Time by Nativity Status (U.S.-Born vs. Immigrant Children), NSCH 2016-2023

.jpg "Laurel E. Wong, BS (she/her/hers) photo")