Session: Mental Health 1: Mental Health in Acute Settings
120 - One Crisis, Two Responses: Comparing Psychiatric Crisis Response Models in a Pediatric Emergency Department
Friday, April 24, 2026
5:30pm - 8:00pm ET
Publication Number: 1110.120
Alexandria N. Lawrence, Monroe Carell Jr. Children's Hospital at Vanderbilt, Nashville, TN, United States; Heather Kreth, Monroe Carell Jr. Children's Hospital at Vanderbilt, Nashville, TN, United States; Erin Johnson, Monroe Carell Jr. Children's Hospital at Vanderbilt, Huntsville, AL, United States; Michele Walsh, Monroe Carell Jr. Children's Hospital at Vanderbilt, FRANKLIN, TN, United States; Ashley Ried, Monroe Carell Jr. Children's Hospital at Vanderbilt, Nashville, TN, United States; Delana Vallery, Monroe Carell Jr. Children's Hospital at Vanderbilt, Nashville, TN, United States; Barron Frazier, Monroe Carell Jr. Children's Hospital at Vanderbilt, Nashville, TN, United States
Resident Physician Monroe Carell Jr. Children's Hospital at Vanderbilt Nashville, Tennessee, United States
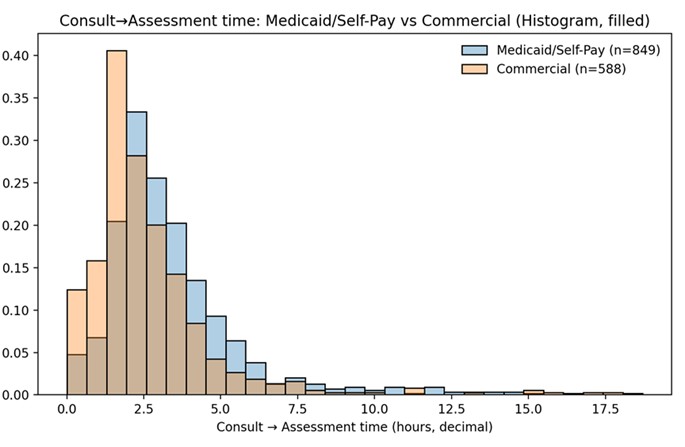
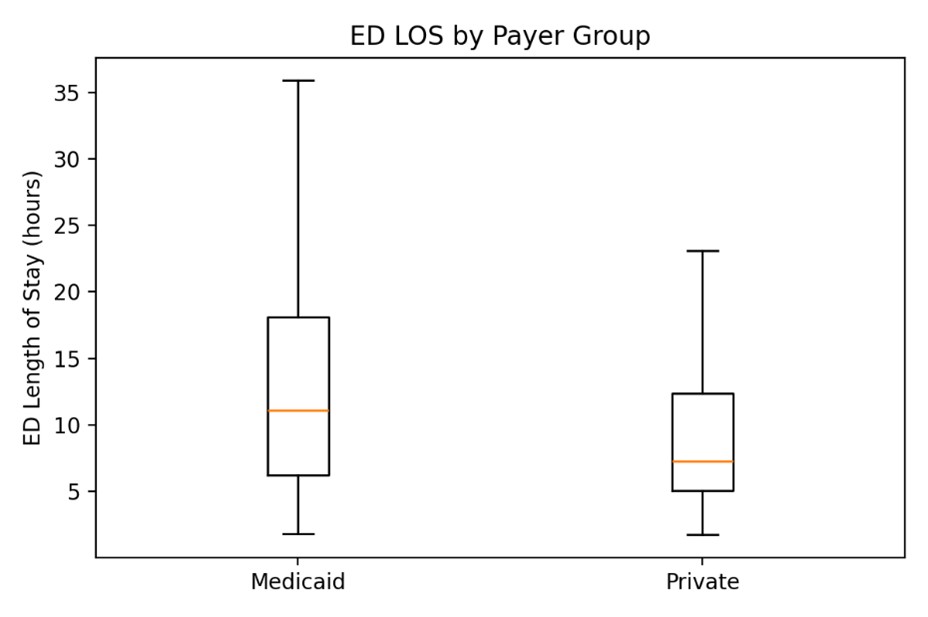
Background: The rate of emergency department (ED) visits for mental health crises continues to rise. Given limited community resources and outpatient treatment centers, the ED has become a primary assessment center for psychiatric crises. At our hospital, psychiatric assessments are based on a child's insurance - a model that exists in certain states. Commercially insured patients are evaluated by an internal psychiatric assessment service, whereas children with Medicaid/Self-Pay are evaluated by a state-contracted community mental health agency. These models differ in their staff training, scope of responsibility, assessment techniques and care pathways. Objective: To determine if systemic differences in psychiatric crisis assessments result in variances in time to assessment, ED length of stay, treatment recommendations and disposition. Design/Methods: A retrospective study was performed on patients under 18 years old who underwent mental health crisis assessment in a pediatric ED at a tertiary children's hospital between July 1, 2024, and June 30, 2025. Patients were excluded if they had a primary medical complaint or if they had a crisis assessment prior to ED arrival. Variables assessed included insurance type, time from psychiatric consult order to completion of assessment, and disposition recommendations (inpatient, outpatient, partial hospitalization, intensive outpatient). Cox proportional hazard models and Chi-Square test were used to compare data distributions. Results: 1437 patients (849 Medicaid/Self-Pay, 588 Commercial) were included in the study. There was a statistically significant difference (p < 0.01) in the time from psychiatric consult order to completion of psychiatric assessment between insurance types, with Medicaid patients waiting an average of 45 minutes longer (Figure 1). Differences in ED length of stay also proved to be significant (p < 0.01), with Medicaid patients staying an average of 4 hours longer, regardless of final disposition (Figure 2). The recommendation for inpatient psychiatric hospitalization was more frequent in Medicaid patients (p=0.0006).
Conclusion(s): Insurance status significantly influences the psychiatric crisis assessment process in the pediatric ED. Patients with Medicaid/Self-Pay experienced longer wait times, extended ED stays and were more likely to receive inpatient recommendations. These disparities highlight the need for more equitable models of care and underscore the role of social determinants in pediatric mental health access.
Time from Psychiatric Consult Order to Completion of Psychiatric
Assessment: Medicaid/Self-Pay vs Commercial Insurance

 photo")