572 - Arriving Fast, Moving Slow: Impact of Mode of Arrival on Emergency Care for Low-Acuity Pediatric Patients
Friday, April 24, 2026
5:30pm - 8:00pm ET
Publication Number: 1549.572
Amanda Seibert, Monroe Carell Jr. Children's Hospital at Vanderbilt, Nashville, TN, United States; Barbara Solomon, Monroe Carell Jr. Children's Hospital at Vanderbilt, Nashville, TN, United States; Barron Patterson, Monroe Carell Jr. Children's Hospital at Vanderbilt, Nashville, TN, United States; Barron Frazier, Monroe Carell Jr. Children's Hospital at Vanderbilt, Nashville, TN, United States
Pediatric Emergency Medicine Fellow Monroe Carell Jr. Children's Hospital at Vanderbilt Nashville, Tennessee, United States
Background: Previous studies estimate that 34-57% of children 15 years and younger who presented to an emergency department (ED) were triaged as an Emergency Severity Index (ESI) 4 or 5. At our institution, patients arriving by ambulance typically bypass the waiting room and are taken directly to an exam room, where triage is performed. Rarely, ambulance arrivals are taken to the waiting room if they are well appearing and the volume is high. We hypothesize that non-urgent visits arriving via ambulance receive different care than similar patients arriving by personal vehicle. Objective: To determine if mode of arrival affected the emergency care time intervals for non-urgent visits. Design/Methods: Retrospective data was collected from July 1, 2022, through June 30, 2025. Patients < 18 years who were triaged as ESI 4 or 5 and discharged were included. Exclusions included outside hospital transfers and patients who left without being seen.
Variables included age, preferred language, insurance, primary care provider status, mode of arrival, time from arrival to provider, time from provider to discharge, and overall length of stay (LOS).
Additionally, we analyzed the time of day that patients were arriving at our ED for non-urgent visits and the average distribution of ambulance vs car arrivals in a 24-hour period.
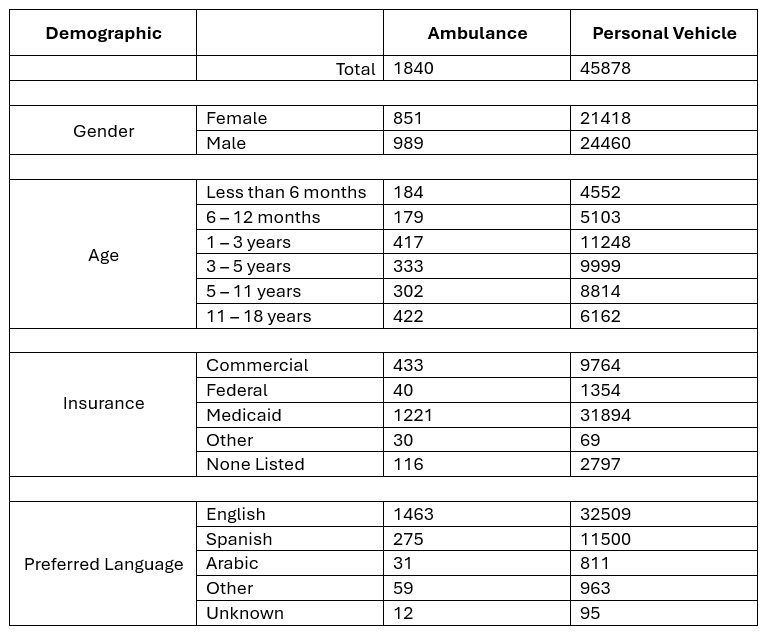
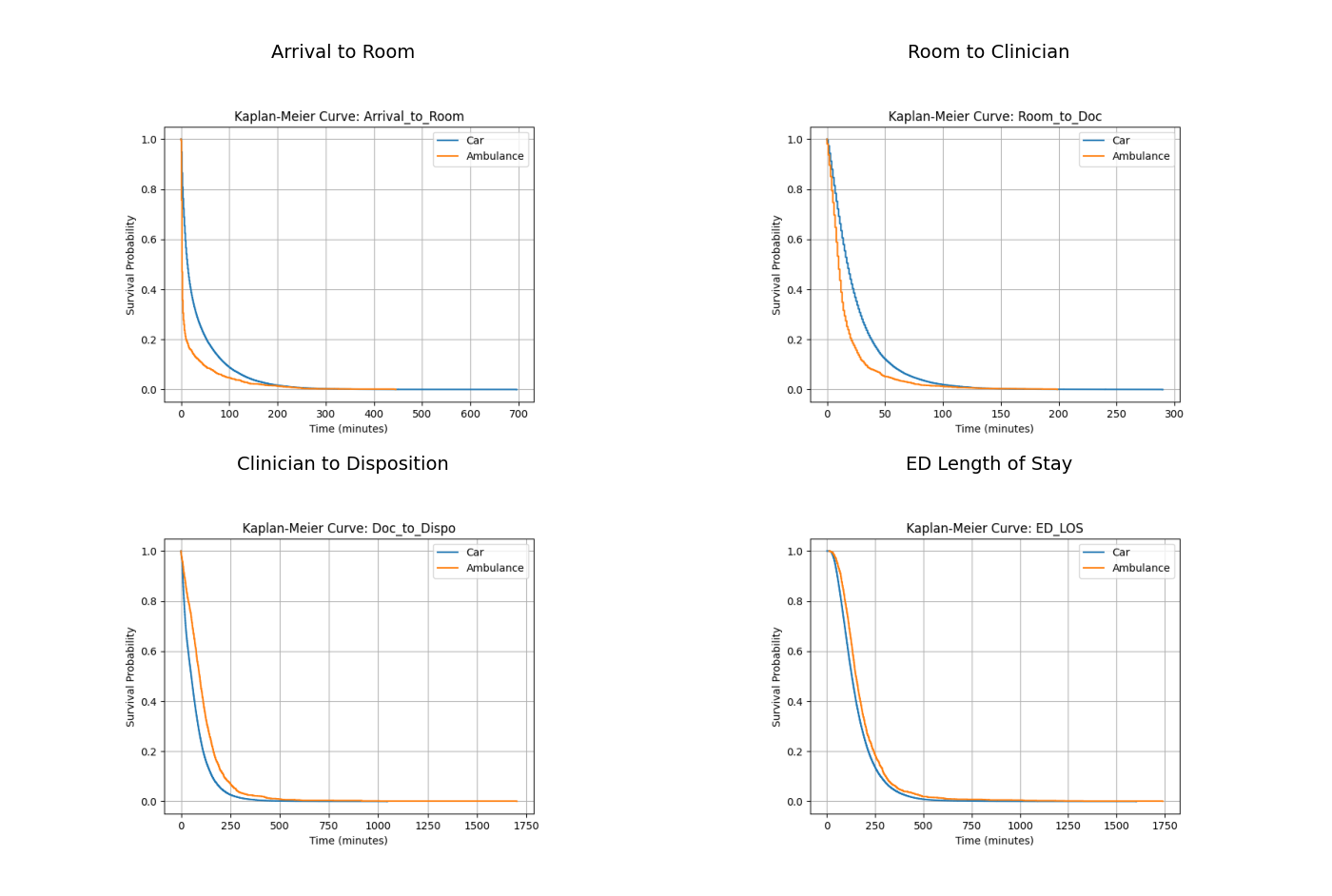
Adjusted Cox proportional hazards were used to compare time intervals and overall length of stay with Kaplan-Meier curve visuals. Covariates included age, language (English vs non-English), and payer. Results: A total of 47,717 encounters were analyzed (Table 1). Most ambulance arrivals of low-acuity visits occurred from 12PM to 6PM, coinciding with peak low-acuity visits. Ambulance arrivals were roomed faster than those arriving by car (HR = 1.98) and saw a provider faster (HR = 1.61). Progression from seeing a provider to disposition was slower in patients arriving by ambulance (HR = 0.683) and had a longer overall LOS (HR = 0.86). All of these were statistically significant with p < 0.001.
Conclusion(s): Non-urgent visits arriving by ambulance have longer ED stays than those arriving by car despite faster rooming and provider evaluation. Low-acuity ambulance arrivals peak at the time when overall low-acuity arrivals also peak in the ED, compounding throughout challenges. These findings suggest that intake design and resource allocation strategies need attention to reduce LOS for low-acuity ambulance arrivals, thereby protecting capacity for higher acuity patients and potentially decreasing left-without-being-seen rates.
Demographic Table Based on Method of Arrival
Kaplan-Meier Survival Curves by Method of Arrival
Time of Day Distribution for Low-Acuity Visits (Ambulance vs Private Vehicle)

 photo")