Session: Neonatal Pulmonology - Clinical Science 2: Bronchopulmonary Dysplasia II
378 - Respiratory Severity Score as a Predictor for Need for Tracheostomy in Infants with Severe Bronchopulmonary Dysplasia
Friday, April 24, 2026
5:30pm - 8:00pm ET
Publication Number: 1362.378
Dinushan C. Kaluarachchi, University of Wisconsin - Madison, Madison, WI, United States; Nethan M. Kaluarachchi, Middleton High School, Middleton, WI, United States; Samuel Afah Annah, University of Wisconsin Madison, Madison, WI, United States; Michael R.. Lasarev, University of Wisconsin School of Medicine and Public Health, Madison, WI, United States; Patrick J. Peebles, University of Wisconsin School of Medicine and Public Health, Madison, WI, United States
Student Middleton High School Middleton, Wisconsin, United States
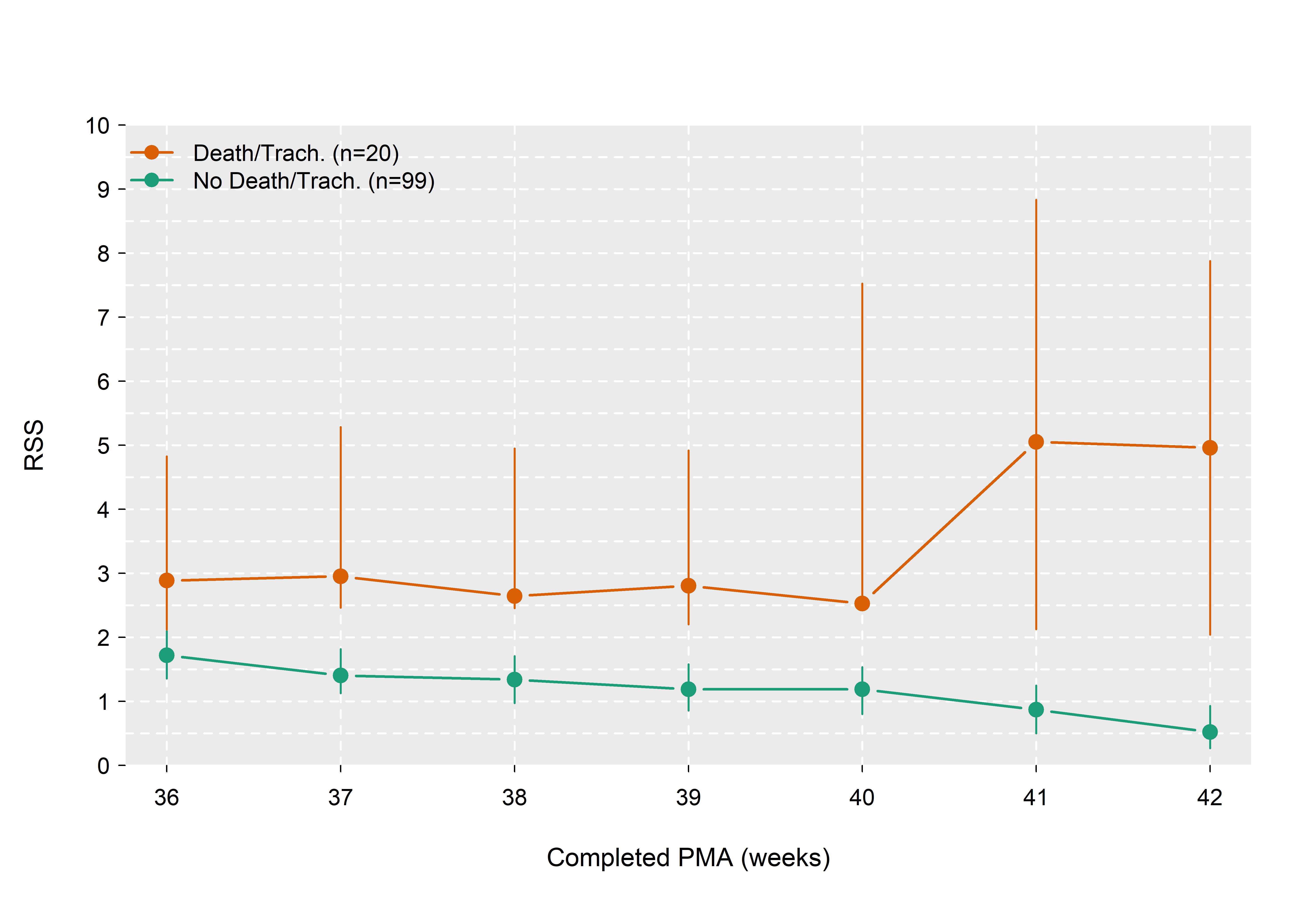
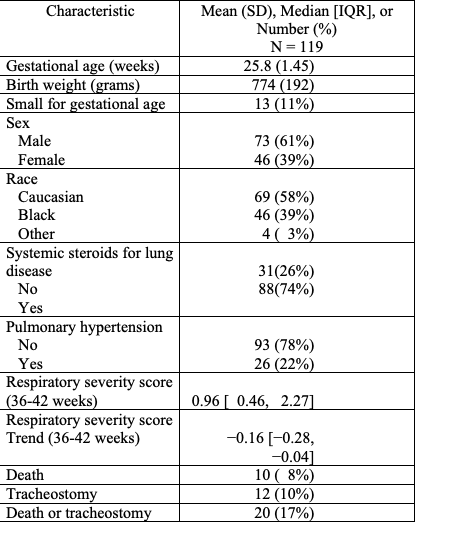
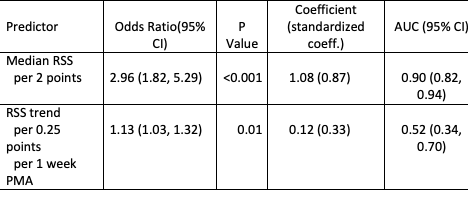
Background: Bronchopulmonary Dysplasia (BPD) is a major sequela of extreme prematurity. A subset of patients with BPD requires tracheostomy placement and chronic ventilatory support. Patient selection and decision-making regarding tracheostomy placement can be challenging. Timely and selective tracheostomy placement in infants with severe BPD can improve lung growth, decrease the need for sedation, and improve the ability to participate in developmental therapies. Objective: To evaluate the association between respiratory severity score (RSS) at 36-42 weeks postmenstrual age (PMA) and need for tracheostomy in extremely preterm infants with severe BPD. Design/Methods: This is a retrospective cohort study of preterm infants born at 230/7 to 286/7 weeks with severe BPD (grade 2 to 3 BPD according to the definition by Jensen et al) in the Prematurity and Respiratory Outcomes Program. Infants with cardiopulmonary anomalies, died prior to 36 weeks' PMA, no BPD or grade 1 BPD and infants with no data on RSS were excluded. Average weekly RSS and RSS trend were calculated for each infant from 36 to 42 weeks. Univariate logistic regression was used to assess whether the average weekly RSS and RSS trend at 36-42 weeks PMA were associated with the primary outcome of death before discharge or tracheostomy placement. Results: A total of 119 infants (89 with grade 2 BPD and 30 with grade 3 BPD) were included in the study. Mean gestational age and birth weight were 25.8 weeks and 774g, respectively. Death before discharge or tracheostomy occurred in 20 (17%) infants (Table 1). Infants who reached the primary outcome had a median RSS of 3.78 (IQR 2.31, 6.38) compared to a median RSS of 0.71 (IQR 0.42, 1.38) among infants without it (Figure 1). Logistic regression revealed that each 2-point increase in median RSS was associated with odds of death or tracheostomy increasing almost 3-fold (OR=2.96; 95% CI: 1.82-5.29, p < 0.001). RSS trend was associated with the primary outcome to a lesser extent (OR=1.13 per 0.25 points per week PMA; 95% CI: 1.03-1.32, p=0.01) (Table 2).
Conclusion(s): Higher average weekly RSS during 36-42 weeks of PMA was associated with odds of death before discharge or tracheostomy placement. Optimal RSS cutoffs for predicting tracheostomy placement need to be determined in large cohort studies.
Figure 1. RSS Distribution for Death/Tracheostomy and No Death/Tracheostomy Cohorts
Table 1. Characteristics of the study cohort
Table 2. Estimated odds ratios (OR) and calculated area under the ROC curve (AUC) from univariable logistic regression analysis.

 photo")