577 - Nurse Practitioner Led Medication Safety of Behavioral Health Patients in the Pediatric Emergency Department
Friday, April 24, 2026
5:30pm - 8:00pm ET
Publication Number: 1554.577
Molly A. Connolly, Boston Children's Hospital, Hanover, MA, United States; Jessica K. Creedon, Boston Children's Hospital, Dover, MA, United States; Debra Lajoie, Boston Children's Hospital, Boston, MA, United States
Emergency Medicine Lead Nurse Practitioner Boston Children's Hospital Hanover, Massachusetts, United States
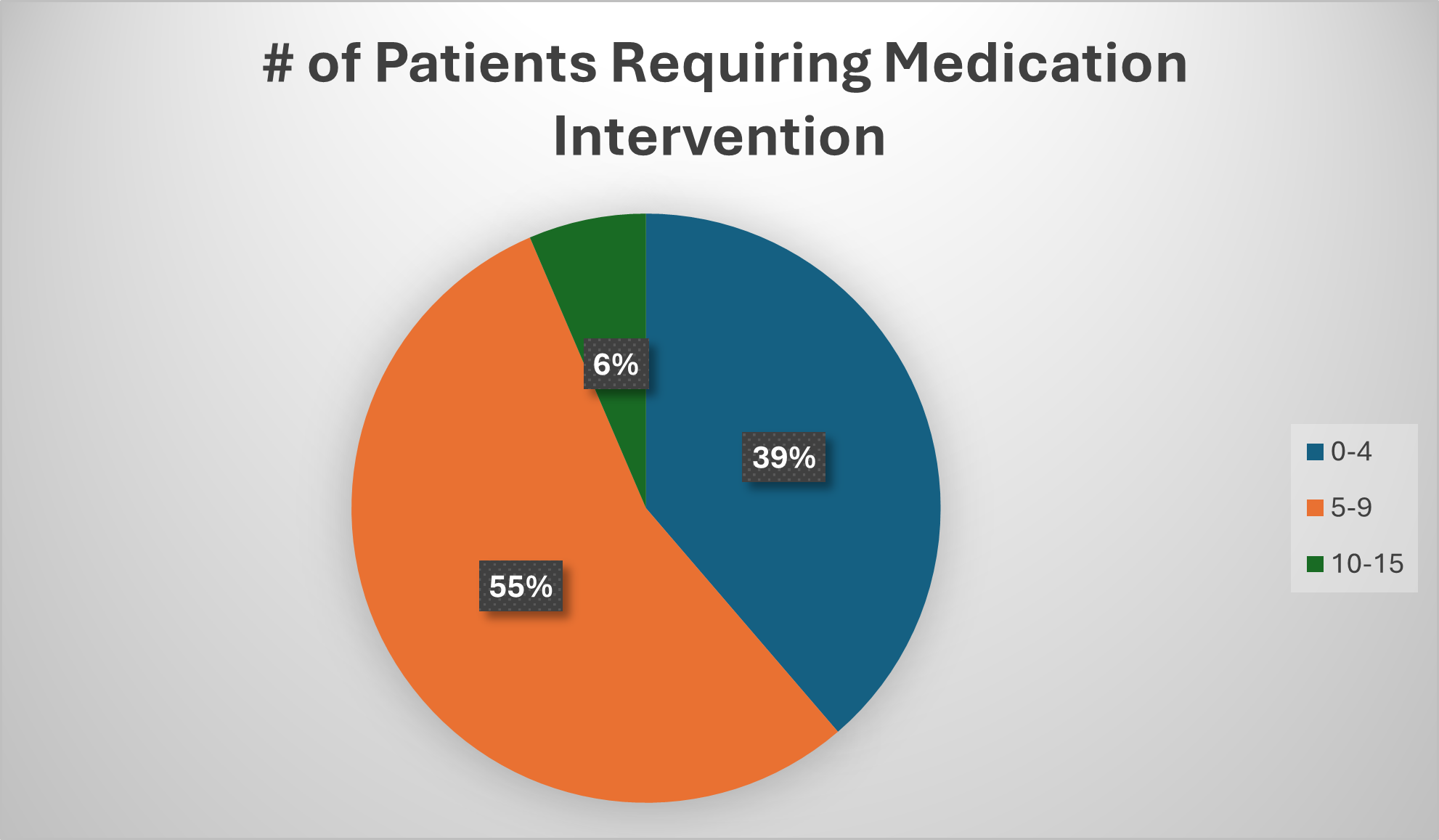
Background: Due to the high volume and complexity of BH patients boarding in the ED with extensive medication lists, a need to design a novel BH NP-led care delivery model was identified to enhance medication safety. Objective: To develop, pilot, and evaluate an NP-led behavioral health medication reconciliation process to improve the accuracy of boarding behavioral health patients' medications. Design/Methods: The smart aim is to perform the ED NP & Pharmacy Medication Safety Huddle on 95% of dayshifts by November 2025. Process Measures include: 1) Reducing the time spent preparing for BH huddles by NPs and pharmacists by 20% by February 2026. 2) Ensure 80% of medication histories are reconciled within 12 hours of ED presentation by February 2026. 3) Enhance the foundational knowledge of BH medications for ED NPs by 20% within six months of implementation. 4) Measure the amount of time the NP and pharmacist pulled from other daily roles and tasks to complete medication history and reconciliation. 5)Describe and characterize the guardianship and residency of the pediatric ED boarding patient population in 90% of daily medication huddles. Balancing measures include measuring the time the NP and the pharmacist spend away from patient care. A Redcap data collection tool is used electronically at the huddle to capture whether the huddle occurred, how many patients required interventions on home medication orders, and the guardianship of the BH patient. Results: The first PDSA cycle demonstrated the model's feasibility and the need for BH medication education. PDSA cycle two is currently in process with data collection through November 1, 2025. Preliminary data analysis shows the huddle occurred on most days despite a large number of patient borders. Over a 34-day period, the huddle occurred 31 days. During this time, there was acuity in the department and NP sick calls.
Conclusion(s): A standardized, daily BH medication huddle improves medication safety and mitigates the risk of withdrawal, behavioral escalations, and restraints, while enhancing patient, family, and staff satisfaction. This intervention can proactively enhance patient safety in high-acuity settings.

 photo")
.png)
