578 - Variation in Emergency Department Experience with Pediatric Critical Illness
Friday, April 24, 2026
5:30pm - 8:00pm ET
Publication Number: 1555.578
Allan M. Joseph, Cincinnati Children's Hospital Medical Center, Cincinnati, OH, United States; Kenneth Michelson, Lurie Children's Hospital, Chicago, IL, United States; Maya Dewan, Cincinnati Children's Hospital Medical Center, Cincinnati, OH, United States; Ellen Lipstein, Cincinnati Children's Hospital Medical Center, Cincinnati, OH, United States; Lynn Babcock, Cincinnati Children's Hospital Medical Center, Cincinnati, OH, United States; Billie S. Davis, University of Pittsburgh School of Medicine, Pittsburgh, PA, United States; Jeremy M.. Kahn, University of Pittsburgh, Pittsburgh, PA, United States
Assistant Professor of Pediatrics Cincinnati Children's Hospital Medical Center Cincinnati, Ohio, United States
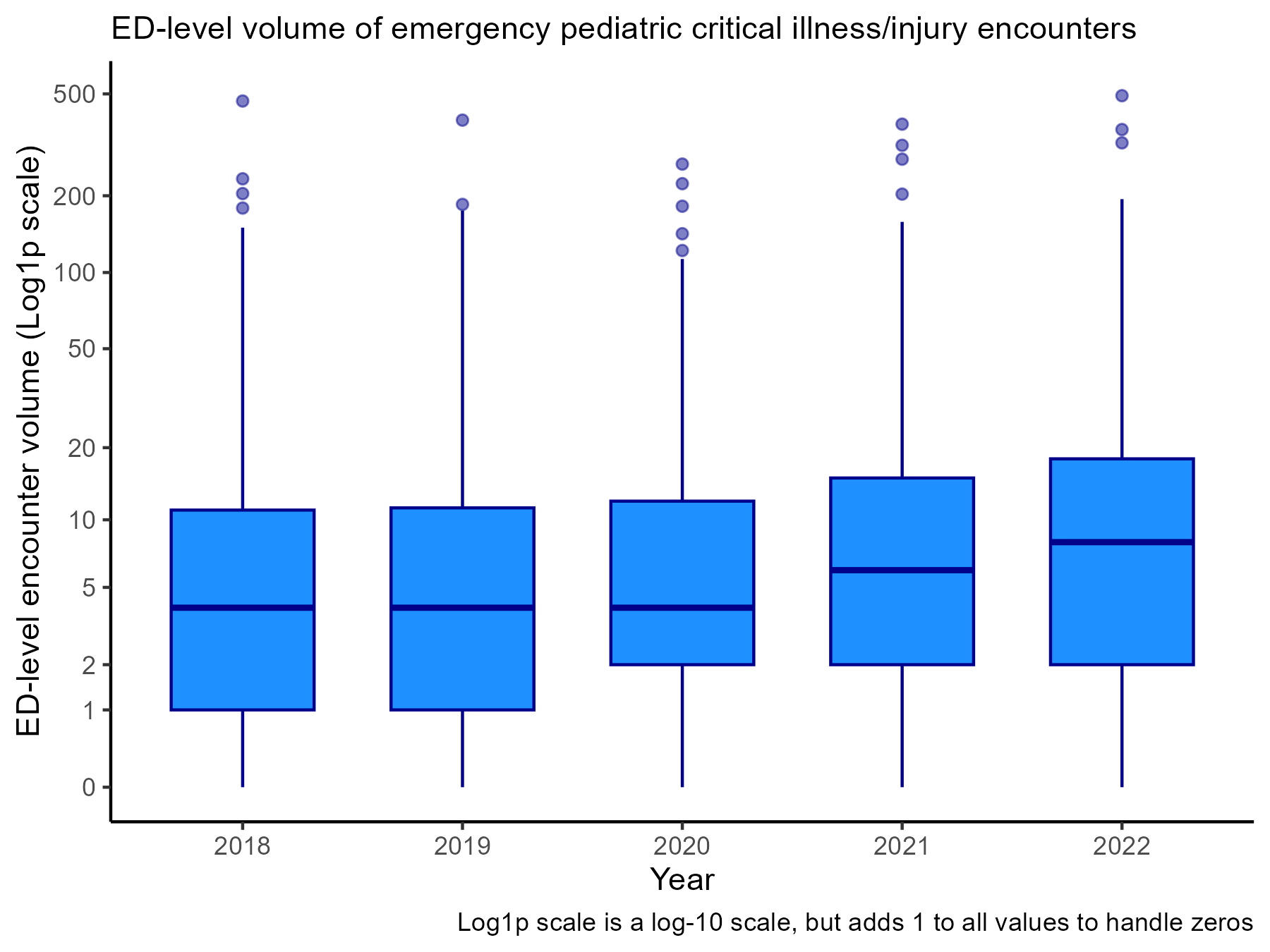
Background: Improving emergency department (ED) pediatric readiness is a national priority. Due to volume-outcome relationships, EDs that rarely care for severely ill children may lack sufficient experience to provide high-quality care, despite investments in pediatric readiness. A better understanding of EDs' experience with pediatric critical illness could help characterize the relative value of broad-based efforts to increase readiness versus direct triage of critically ill children to high-volume EDs. Objective: To quantify how often EDs encounter pediatric critical illness and evaluate the proximity of these encounters to a nearby high-volume ED. Design/Methods: We studied the United States Healthcare Cost & Utilization Project State Emergency Department and State Inpatient Databases from Florida, Iowa, Maryland, Nebraska, and Wisconsin from 2018-2022. We defined critically ill children as patients under 18 years old who experienced ED death, cardiopulmonary resuscitation, endotracheal intubation, or billing for critical care services. We then quantified variation in caseload across EDs, as well as the proportion of patients that could have alternatively been seen in a high pediatric volume ED (an ED in the top quartile of volume within 15 minutes' drive of the patient's home or index ED, as calculated in ArcGIS Pro). Results: In our primary analysis, we identified 569 EDs and 39,727 emergency pediatric critical illness encounters. The median ED treated 5 critically ill children each year (interquartile range [IQR] 1 - 14), plotted on a logarithmic scale by year in the Figure. 181 (31.8%) EDs had at least one year in which they treated zero critically ill children. Of the 9,102 encounters not in high-volume EDs, 1,509 (16.6%) could have occurred in a nearby high-volume ED. These proportions varied by state (Table).
The results were similar when we expanded our definition of critical illness to include all children admitted to an ICU within one day following an ED visit (n= 214,170). In this analysis, the median ED treated 12 patients each year (IQR 4 - 36), and 84 (14.8%) EDs had at least one year in which they treated no critically ill children. Of the 22,428 encounters under the expanded definition not in high-volume EDs, 4,076 (18.2%) could have occurred in a nearby high-volume ED.
Conclusion(s): Most EDs see few critically ill children, and some of these encounters could be diverted to nearby high-volume EDs. Diversion may improve emergency care in some areas, but in other areas it may be necessary for all EDs to be fully prepared for pediatric emergencies.
Figure: ED-level volume of emergency pediatric critical illness encounters over time
Table. Variation in ED-level caseload of critically ill children, by state.

 photo")
.png)
