580 - Disaster Networking Collaborative: Building Sustainable Pediatric Disaster Preparedness Across U.S. Children’s Hospitals
Friday, April 24, 2026
5:30pm - 8:00pm ET
Publication Number: 1557.580
Jonathan R. Eisenberg, University of Texas at Austin Dell Medical School, Austin, TX, United States; Julie A.. Shelton, University of Texas at Austin Dell Medical School, Weaverville, NC, United States; Laura D.. Aird, University of Texas at Austin Dell Medical School, Austin, TX, United States; Brent D. Kaziny, Texas Children's Hospital, Houston, TX, United States; Katherine Remick, University of Texas at Austin Dell Medical School, Austin, TX, United States
Assistant Professor University of Texas at Austin Dell Medical School Austin, Texas, United States
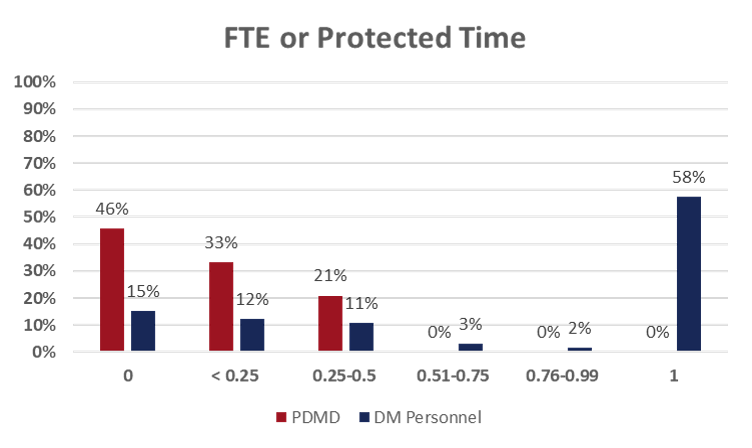
Background: Children are disproportionately affected by disasters, yet pediatric disaster preparedness is often underdeveloped. To address this gap, the Pediatric Pandemic Network (PPN) launched the Disaster Networking Collaborative (DNC) to improve pediatric disaster preparedness across US children's hospitals. The Institute for Healthcare Improvement's Breakthrough series collaborative model was used to accelerate change, enhance sustainability, and promote knowledge sharing across diverse teams. The DNC focused on promoting children's hospitals as leaders and advocates to support collaboration with community hospitals, healthcare coalitions, and other community-based entities engaged in planning and response efforts. Objective: We sought to evaluate whether a national collaborative could improve pediatric disaster preparedness initiatives within children's hospitals. Design/Methods: Planning began in November 2022 where an advisory committee developed collaborative materials and content. Baseline, mid, and post-collaborative surveys captured demographics, institutional resources, leadership support, previous disaster management education/training, and implementation of preparedness initiatives. Hospital based teams participated in monthly learning sessions over the course of 10 months addressing C-suite commitment and support, standardized disaster roles, and integration into local/state response networks. Results: Of 102 hospitals registered, 72 (67%) completed the baseline scan, representing 291 individuals (29% physicians, 27% nurses, 15% emergency managers). Holding an MD/DO degree made up 29% of respondents, followed by RN with 27%. Most institutions had limited pediatric disaster medical director (PDMD) support ( < 0.25 full time equivalent [FTE] in 79%), compared with fully funded (1.0 FTE) emergency manager roles (58%).
Conclusion(s): The DNC demonstrated that targeted collaborative initiatives can significantly advance foundational pediatric disaster preparedness, even in the absence of formal mandates or funding. But sustained investment is needed to scale and institutionalize these gains within children's hospitals.

 photo")