Session: Neonatal Pulmonology - Clinical Science 1: Bronchopulmonary Dysplasia I
364 - Prediction model of severe bronchopulmonary dysplasia using objective indicators: a multicenter prospective cohort study in Japan
Friday, April 24, 2026
5:30pm - 8:00pm ET
Publication Number: 1348.364
Seiichi Tomotaki, Kyoto University Hospital, Kyoto, Kyoto, Japan; Ryosuke Araki, Kyoto University Hospital, Kyoto, Kyoto, Japan; Katsuya Hirata, Osaka Women's and Children's Hospital, Izumi, Osaka, Japan; Katsuaki Toyoshima, Kanagawa children's Medical Center, Yokohama, Kanagawa, Japan; Tetsuya Isayama, National Center for Child Health and Development, Setagaya-ku, Tokyo, Japan; Ryo Ogawa, Nagano Children's Hospital, Azumino, Nagano, Japan; Hiroko Ishii. Iwami, Osaka City General Hospital, Osaka, Osaka, Japan; Toshifumi Ikeda, Aomori Prefectural Central Hospital, Aomori, Aomori, Japan; Hirokazu Arai, Akita Red Cross Hospital, Akita, Akita, Japan; Akari Makidono, Tokyo Metropolitan Children's Medical Center, Fuchu, Tokyo, Japan; Masanori Nishikawa, Osaka Women's and Children's Hospital, Sakai, Osaka, Japan; Mikiko Miyasaka, National Center for Child Health and Development, Setagaya-ku, Tokyo, Japan; Hiroko Hara, Kurashiki Central Hospital, Kurashiki, Okayama, Japan; Yu Hidaka, Kyoto University, Sakyo-ku,Shogoin,Kataharamachi, Kyoto, Japan; Masahiko Kawai, Kyoto University, Kyoto, Kyoto, Japan
Associate Professor Kyoto University Hospital Kyoto, Kyoto, Japan
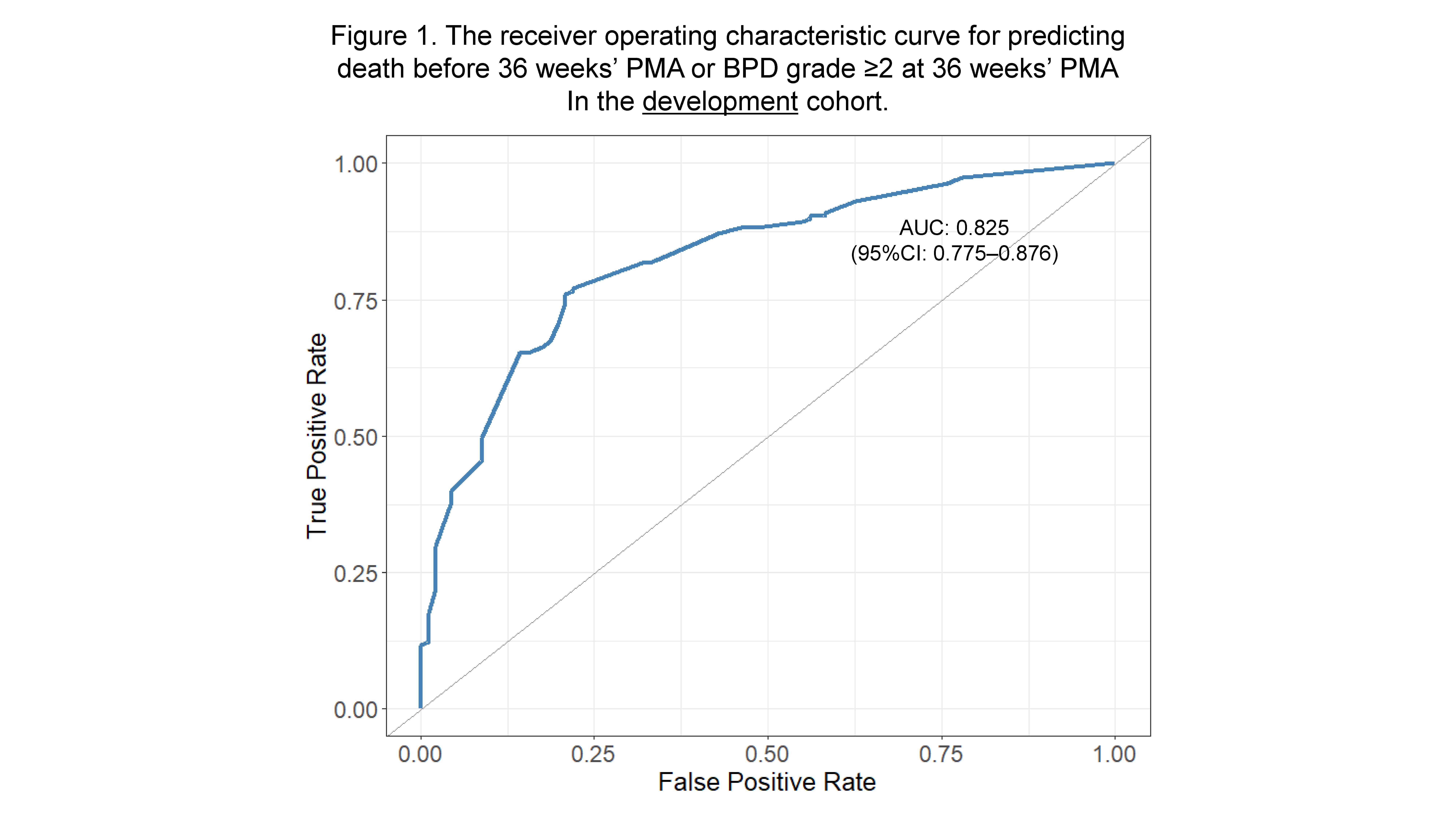
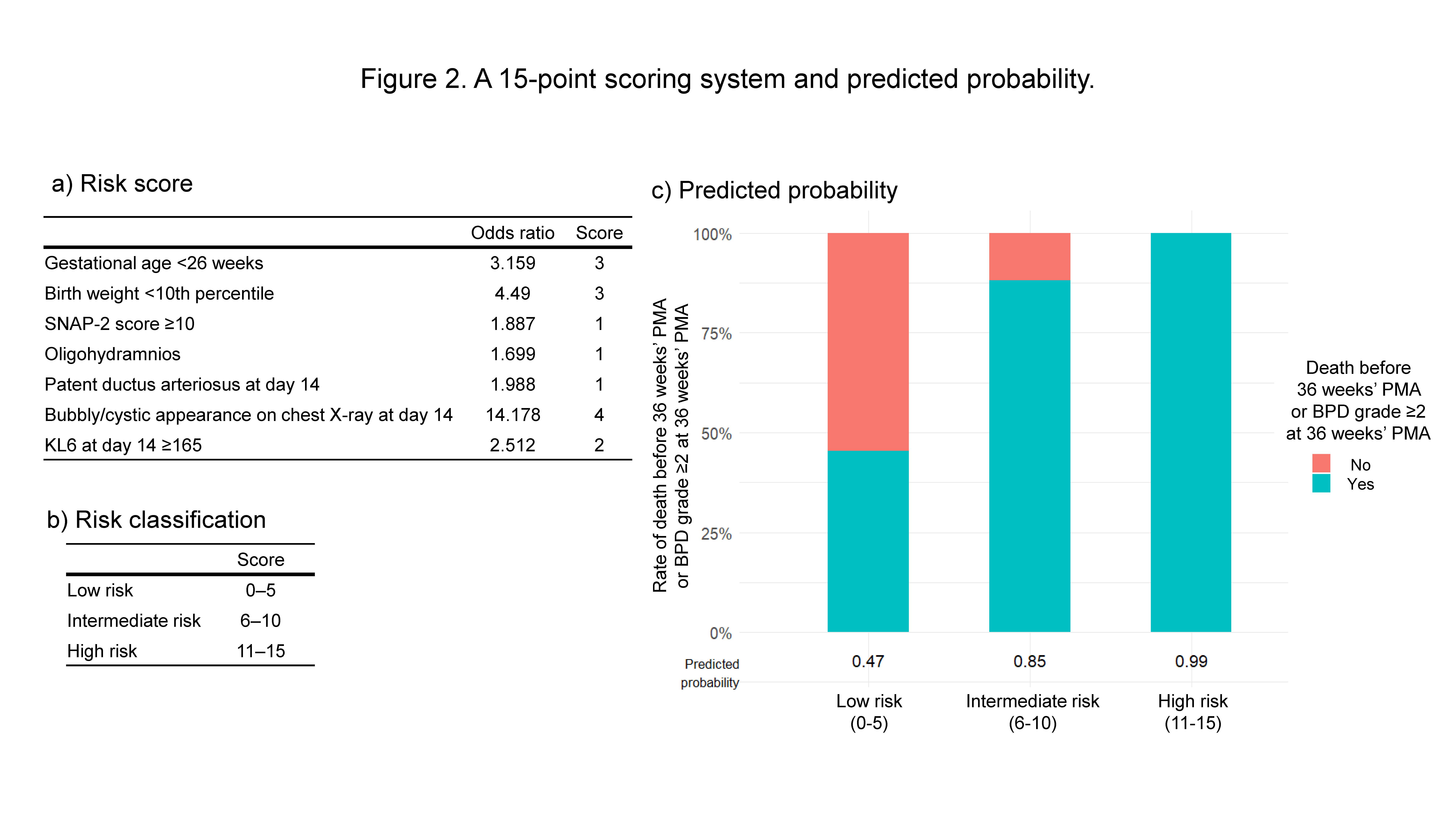
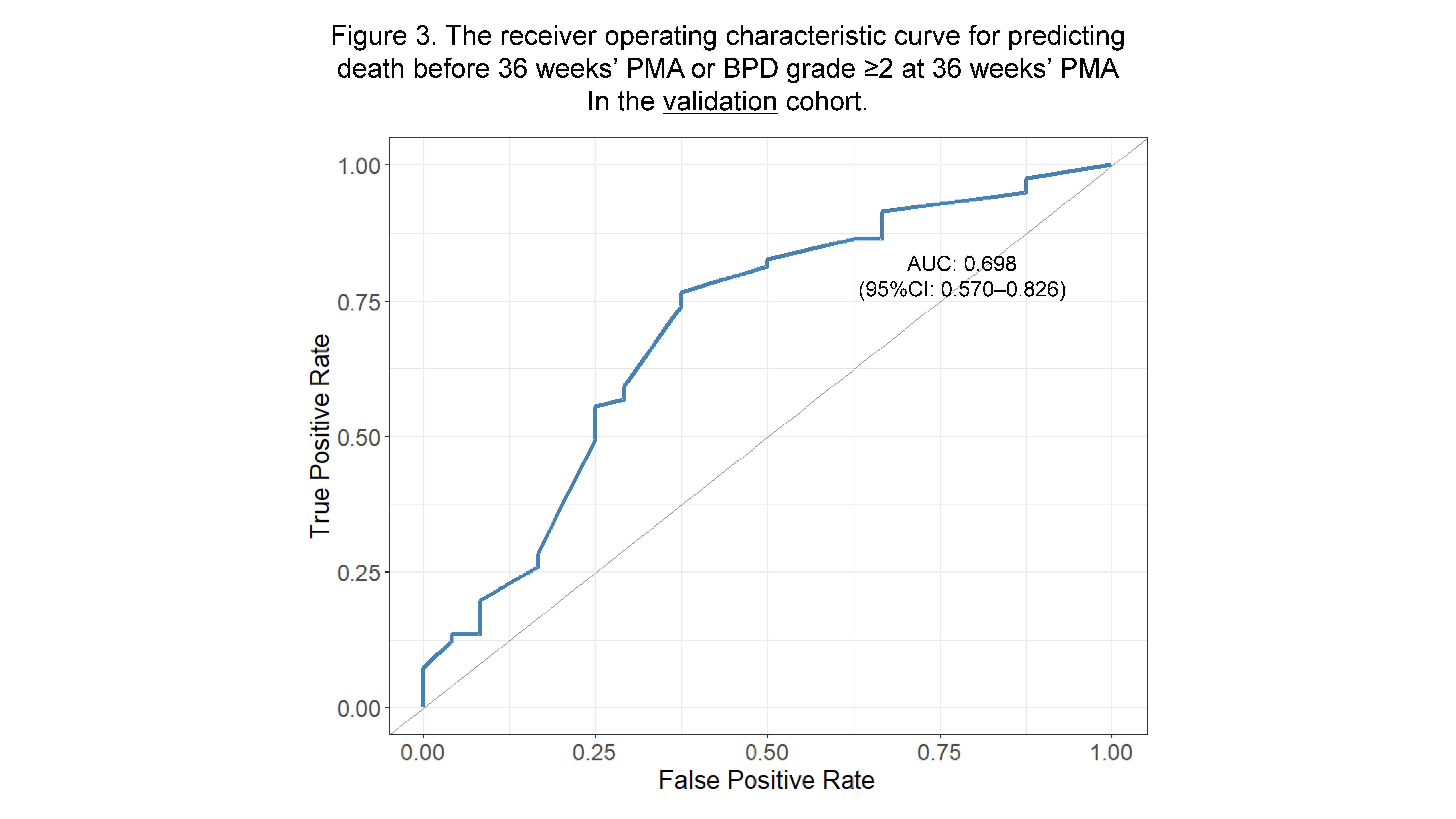
Background: Since severe bronchopulmonary dysplasia (BPD) affects the long-term prognosis of preterm infants, early prediction of its onset is crucial for prevention. Several prediction models for severe BPD have been reported, but few rely solely on objective indicators that are independent of clinical management or treatment strategies. Objective: This study aimed to develop a prediction model for severe BPD using only objective indicators independent of management policies, based on a multicenter prospective cohort in Japan. Design/Methods: This multicenter cohort study included preterm infants born at ≤28 weeks' gestation. Infants born between July 2020 and June 2022 were used to develop a model predicting death before 36 weeks' postmenstrual age (PMA) or BPD grade ≥2 at 36 weeks' PMA. Validation was performed using infants born between July 2022 and June 2023. Variables were selected from previously reported predictors according to the following criteria: 1) available within the first 14 days of life, 2) objective and highly generalizable, 3) independent of treatment or management strategies, and 4) significantly associated (high odds ratio) in univariate logistic regression analysis. Multivariate logistic regression analysis was performed, and the area under the receiver operating characteristic curve (ROC-AUC) was calculated. A 15-point scoring system was created based on the odds ratios. This study was approved by the ethics committee of each participating institute. Results: A total of 535 infants from nine facilities were enrolled, with 473 eligible for analysis after exclusions (development cohort: 331; validation cohort: 142). Seven variables-gestational age, small for gestational age (birth weight < 10th percentile), oligohydramnios, SNAP-II score, patent ductus arteriosus at day 14, bubbly/cystic appearance on chest X-ray at day 14, and serum KL-6 at day 14-were selected for the prediction model, which had an ROC-AUC of 0.825 (95% confidence interval [CI]: 0.775-0.876). The predicted probability of the outcome was 47% for scores ≤5, 85% for scores of 6-10, and 100% for scores ≥11. In the validation cohort, the ROC-AUC was 0.698 (95% CI: 0.570-0.826).
Conclusion(s): We developed a model to predict death or BPD grade ≥2 using objective indicators obtained within the first 14 days of life, independent of treatment strategies. This model demonstrated good performance in the validation cohort and may be useful for risk stratification in clinical practice.
Figure 1. The receiver operating characteristic curve for predicting death before 36 weeks' PMA or BPD grade ≥2 at 36 weeks' PMA In the development cohort.
Figure 2. A 15-point scoring system and predicted probability.
Figure 3. The receiver operating characteristic curve for predicting death before 36 weeks' PMA or BPD grade ≥2 at 36 weeks' PMA In the validation cohort.

 photo")