678 - Retrospective Review of Neonates with Non-IgE-Mediated Cow’s Milk Allergy Compared to Those with Necrotizing Enterocolitis Hospitalized in the Neonatal Intensive Care Unit
Friday, April 24, 2026
5:30pm - 8:00pm ET
Publication Number: 1655.678
Alexandra N. Kaplan, University of Rochester School of Medicine and Dentistry, Rochester, NY, United States; Jonathan Burris, University of Rochester School of Medicine and Dentistry, Rochester, NY, United States; Amy D. Burris, Golisano Children's Hospital at The University of Rochester Medical Center, Rochester, NY, United States; Hongyue Wang, University of Rochester School of Medicine and Dentistry, Rochester, NY, United States; Kirsi Jarvinen-Seppo, Golisano Children's Hospital at The University of Rochester Medical Center, Rochester, NY, United States
Medical Student University of Rochester School of Medicine and Dentistry Rochester, New York, United States
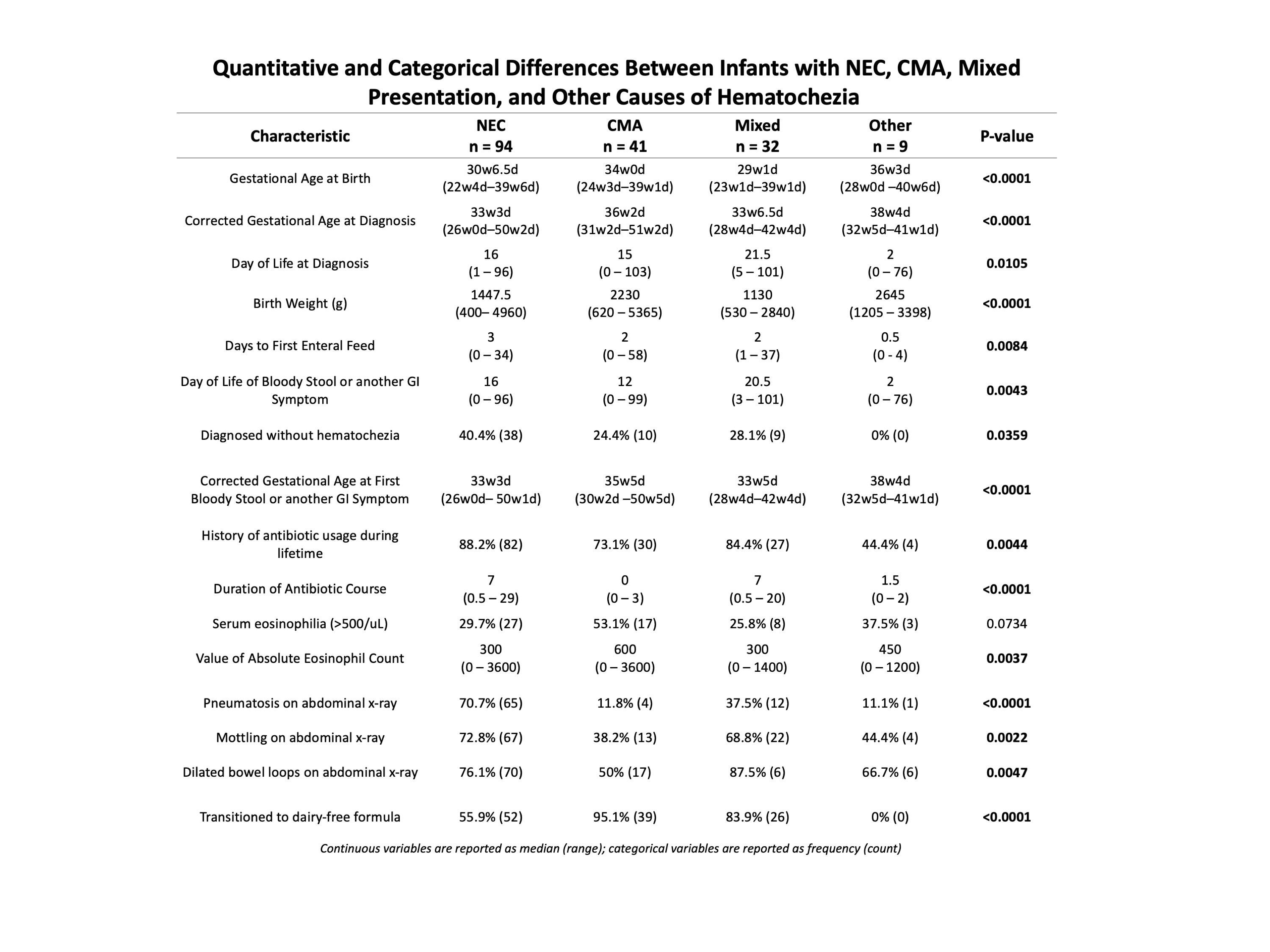
Background: Hematochezia in neonates merits evaluation given risk for life-threatening diseases such as necrotizing enterocolitis (NEC), septic ileus, and midgut volvulus. However, when the clinical picture and evaluation do not indicate intestinal ischemia, enterocolitis, or infection, non-IgE-mediated cow's milk allergy (CMA) should be considered. CMA is a food allergy increasingly recognized in both preterm and term neonates, though its incidence and clinical characteristics in the premature neonate remain poorly defined. Objective: This study investigated through a retrospective chart review whether CMA and NEC differ or overlap in clinical presentation, laboratory findings, and imaging to characterize the incidence of CMA in a level IV neonatal intensive care unit (NICU). We hypothesized that term and preterm neonates develop CMA due to exposure to cow's milk protein in breast milk and formula. Design/Methods: Charts from 176 neonates admitted to the University of Rochester NICU from 2017 to 2023 diagnosed with NEC, CMA, or other hematochezia were reviewed. Patients born at 22 weeks gestation (GA) to 42 weeks GA were categorized into: NEC, CMA, mixed presentation, or other diagnoses. Kruskal-Wallis, chi-square, and Fisher's exact tests analyzed between-group differences in neonatal birth/medical history, timing of presentation, feeding practices, imaging, serum eosinophilia, and treatment. Results: 162 pre-term and 14 full-term infants were included and categorized as NEC (n=94), CMA (n=41), mixed NEC and CMA (n=32), or other diagnoses (n=9). Differences between groups existed for gestational age at birth and at diagnosis (p < 0.0001), birth weight (p < 0.0001), days to first enteral feed (p=0.0084), days to first symptom (p=0.0043), nutrition source at presentation (p < 0.0001), duration of antibiotic course (p < 0.0001), presence of mottling, bowel dilation, and pneumatosis on imaging (p=0.0003, p=0.0049, p< 0.0001), and serum eosinophilia (p=0.0173). Birth weight, gestational age at birth, and absolute serum eosinophils were highest in CMA. Nutritional management differences existed with transition to hydrolyzed formula (p < 0.0001) and nutrition source at discharge (p=0.0225). Additionally, 13 of the patients with a mixed presentation experienced multiple episodes of hematochezia or other gastrointestinal symptoms.
Conclusion(s): Premature neonates experience CMA with key differences from those with NEC in clinical presentation, imaging results, and serum eosinophilia. Mixed presentations raise questions about coexisting pathology and indicate the need for diagnostic point-of-care markers for CMA in the NICU.
Quantitative and Categorical Differences Between Infants with NEC, CMA, Mixed Presentation, and Other Causes of Hematochezia
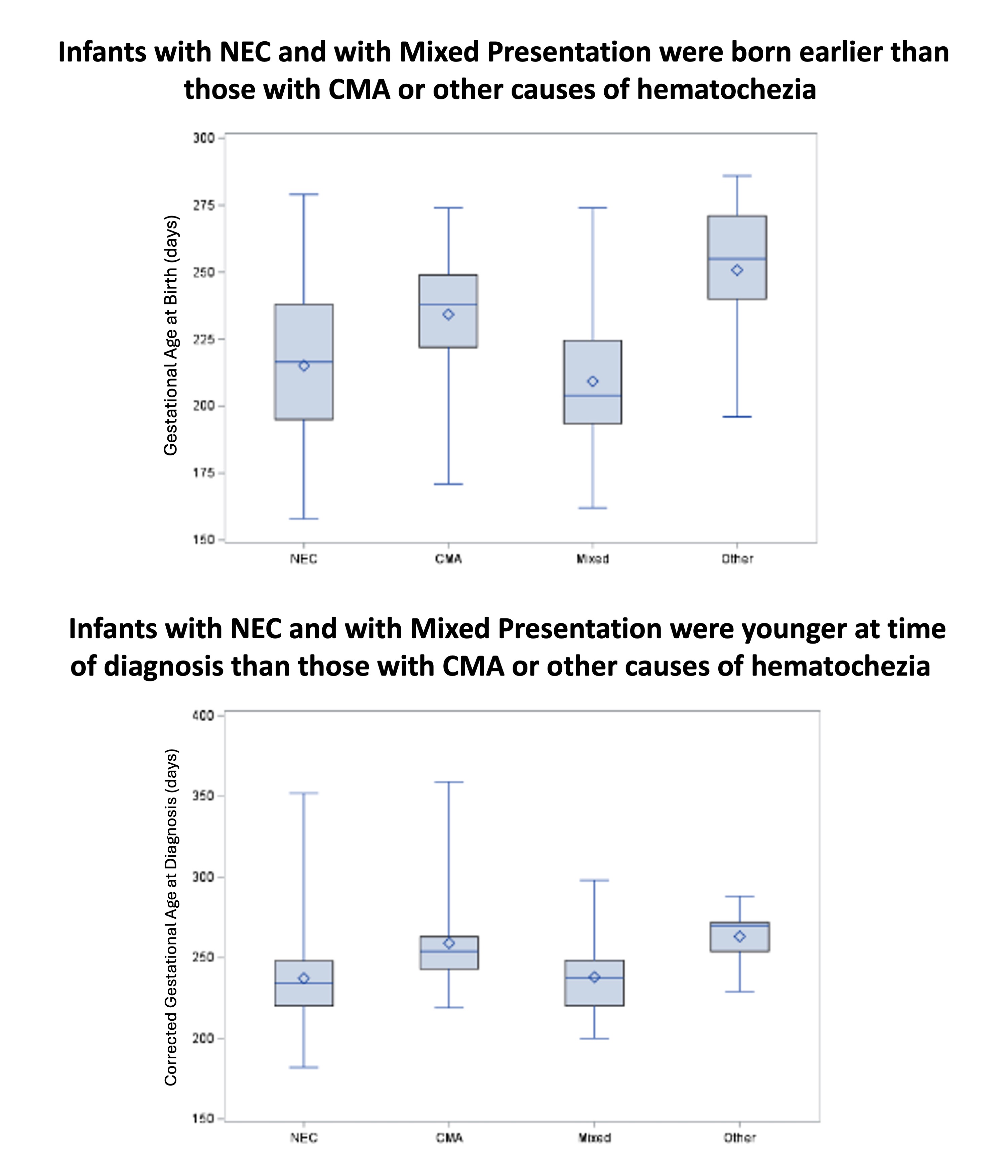
Infants with NEC and Mixed Presentation Were Born and Diagnosed Earlier Than Those with CMA or Other Causes of Hematochezia
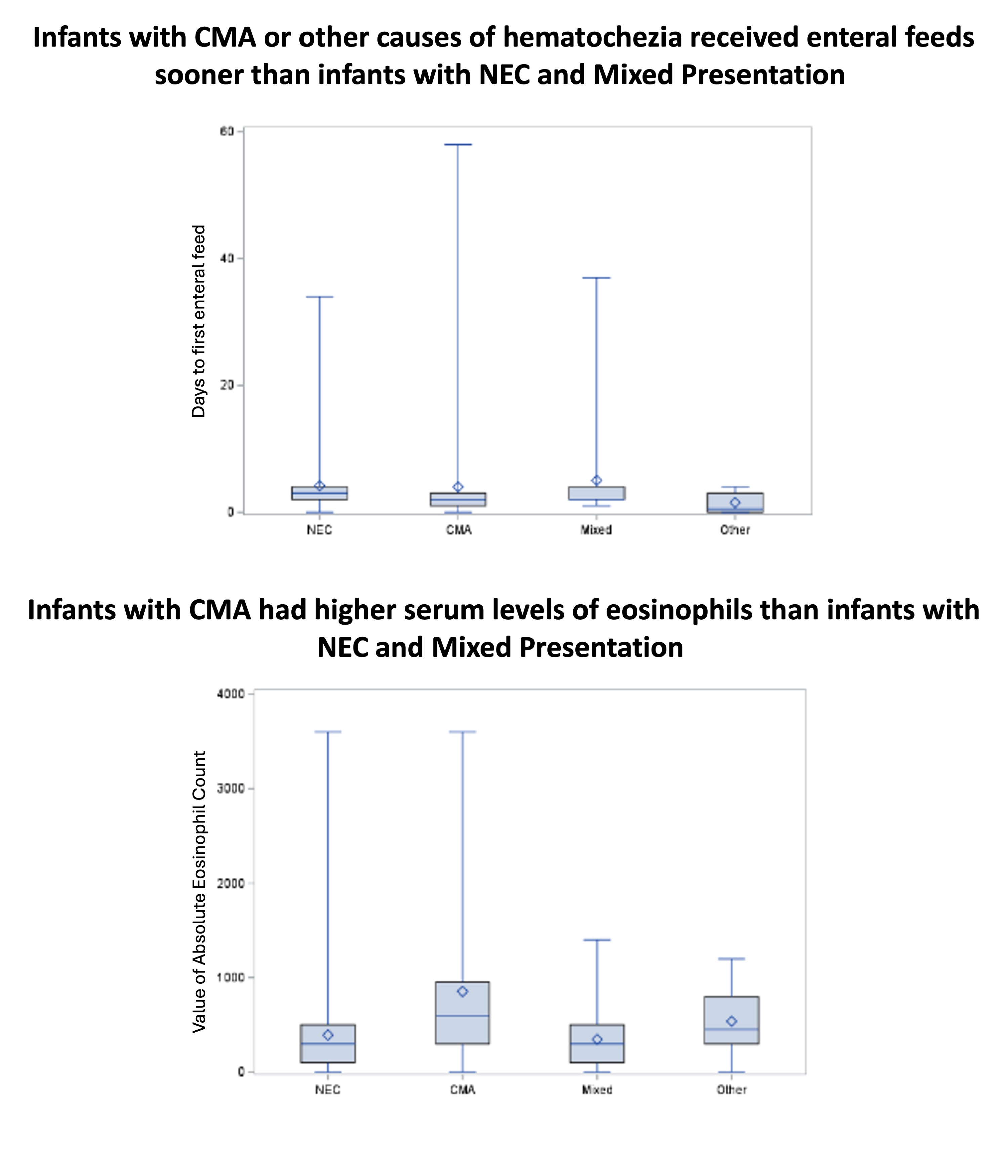
Infants with CMA Had Earlier Enteral Feeding and Higher Serum Eosinophils Compared with NEC and Mixed Presentation

 photo")