64 - School age survival, neurodevelopment and health outcomes after moderate-severe HIE: a population cohort study
Friday, April 24, 2026
5:30pm - 8:00pm ET
Publication Number: 1057.64
Philippa Rees, UCL Great Ormond Street Institute of Child Health, London, England, United Kingdom; Chris Gale, Imperial College London, London, England, United Kingdom; Cheryl Battersby, Imperial College London, London, England, United Kingdom; Alastair Sutcliffe, UCL Great Ormond Street Institute of Child Health, London, England, United Kingdom; Ben Carter, King's College London, London, England, United Kingdom
NIHR Doctoral Fellow UCL Great Ormond Street Institute of Child Health London, England, United Kingdom
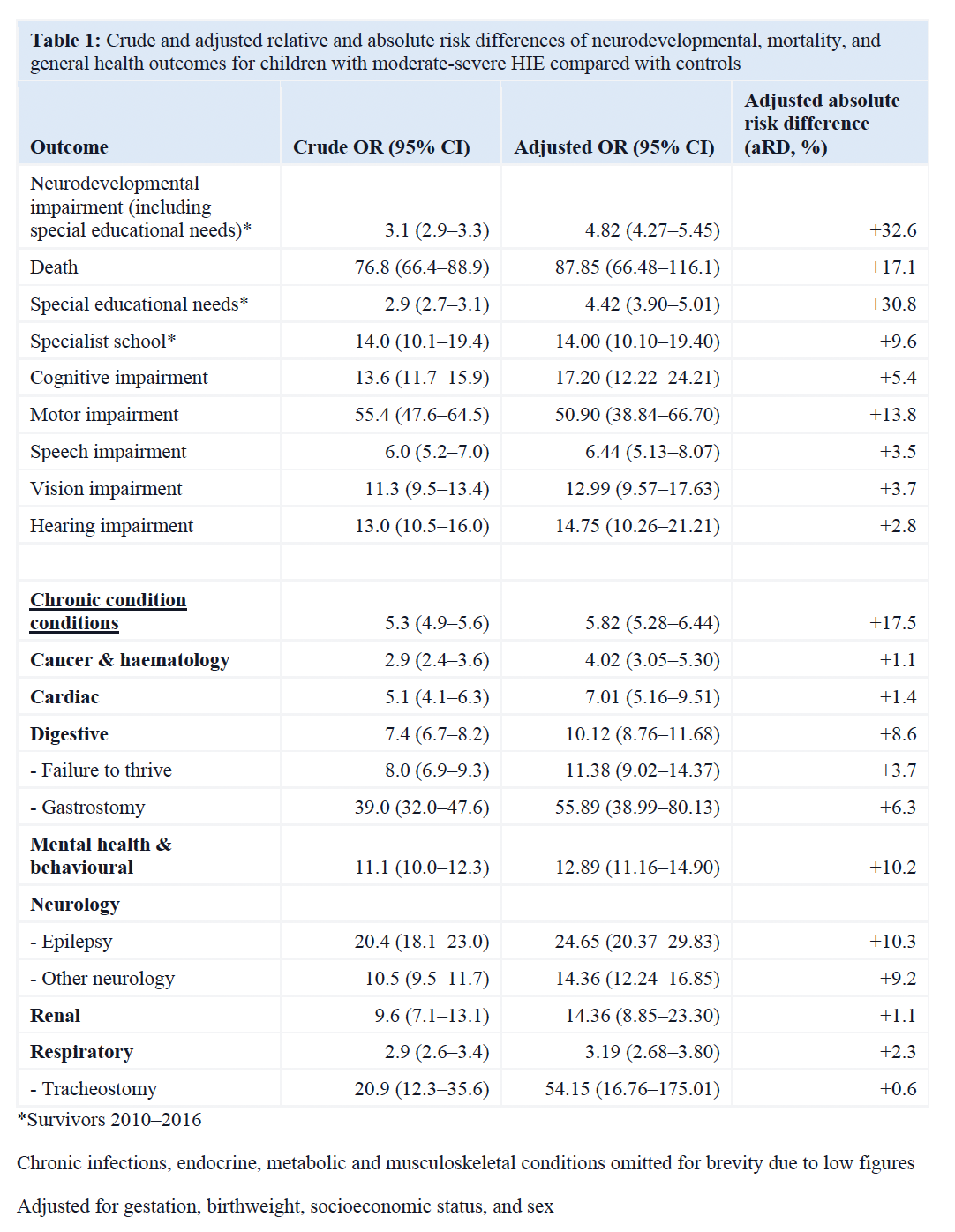
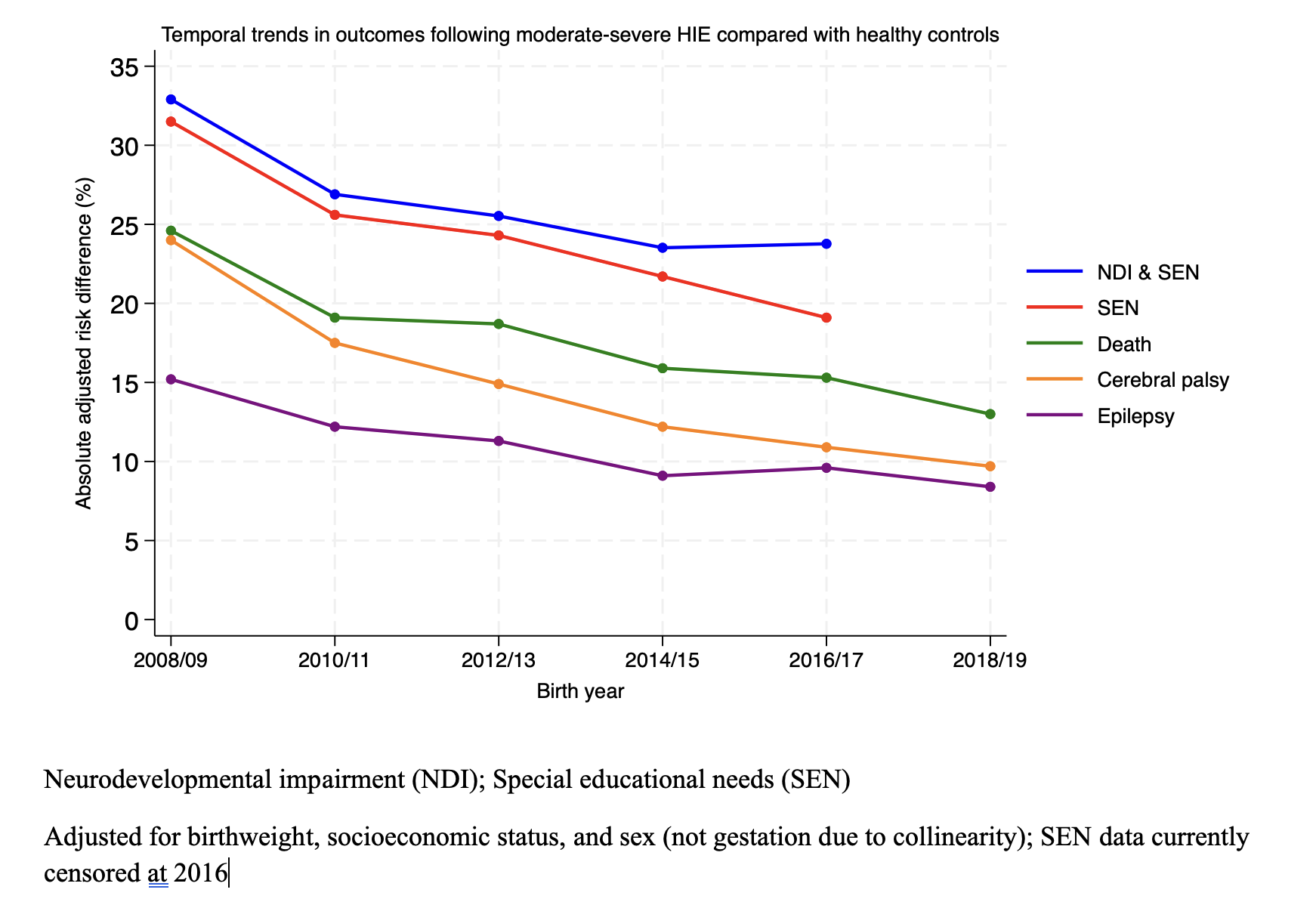
Background: Since the adoption of therapeutic hypothermia for moderate-severe HIE; comprehensive, national, population‑level data on long‑term childhood health and educational outcomes are lacking. Objective: To determine neurodevelopmental, mortality, general health, and educational outcomes up to 13 years of age in babies ≥36 weeks' gestation with moderate-severe HIE in England between 2008-2019 compared to healthy controls. Design/Methods: We performed a population cohort study using linked data from the CHERuB study (which includes National Neonatal Research Database (NNRD), national health, school and social care data). Babies with moderate-severe HIE were identified from diagnostic, clinical, and physiological data in the NNRD. Children were followed to 13 years, October 2024, or death (mean 9 years); with follow-up data available for 96.6% of children. Primary outcomes included survival with neurodevelopmental impairment (NDI) including special educational needs (SEN); mortality; and chronic health conditions. Crude and adjusted risks and adjusted absolute risk differences (aRDs) were estimated using multivariable logistic regression. Results: 9,827 infants with moderate-severe HIE and 74,781 controls were included. In the HIE group median umbilical arterial base excess was −9.3 mmol/L, median arterial cord pH was 7.02 and median 10‑minute Apgar was 7. Neonatal seizures occurred in 56.8%. HIE survivors had an adjusted absolute risk difference (aRD) for NDI or SEN of 32.6%, largely driven by cerebral palsy (aRD 13.8%) and SEN (aRD 30.8%) (Table 1). The aRD for childhood death versus controls was 17.1%. Most deaths (80.8%) occurred on the neonatal unit; with a median time-to-death on the unit of 2.7 days. Mortality fell from an aRD of 24.6% to 13.0% between 2008/9 and 2018/19 (Figure 1). Survivors had an aRD of 17.5% for any chronic childhood condition, including epilepsy (aRD 10.3%), mental health and behavioural disorders (aRD 10.2%), and gastrointestinal problems (aRD 8.6%) such as having a gastrostomy (aRD 6.3%). Most survivors attended mainstream school; the aRD for attending a specialist school was 9.6%. The aRDs for NDI, SEN, death, cerebral palsy and epilepsy decreased between 2008 and 2019 (Figure 1).
Conclusion(s): Outcomes of children with moderate-severe HIE have improved markedly. However, a substantial proportion of survivors continue to have NDI or require SEN support (aRD 23.8% in 2016). This study-large enough to provide precise, contemporary population‑level estimates-gives clinicians and families better information to guide counselling and to prepare for the future.
Table 1: Crude and adjusted relative and absolute risk differences of neurodevelopmental, mortality, and general health outcomes for children with moderate-severe HIE compared with controls
Temporal trends in outcomes following moderate-severe HIE compared with healthy controls

 MPhil MBBCh MRCPCH photo")