415 - An Innovation for the Automated Collection and Analysis of Multicenter Ambulatory Blood Pressure Monitoring Data at Scale: The SUPERHERO ABPM Phase
Friday, April 24, 2026
5:30pm - 8:00pm ET
Publication Number: 1398.415
James T. Nugent, Yale School of Medicine, New Haven, CT, United States; Andrew M.. South, Wake Forest School of Medicine of Wake Forest Baptist Medical Center, Winston Salem, NC, United States
Assistant Professor of Pediatrics Yale School of Medicine New Haven, Connecticut, United States
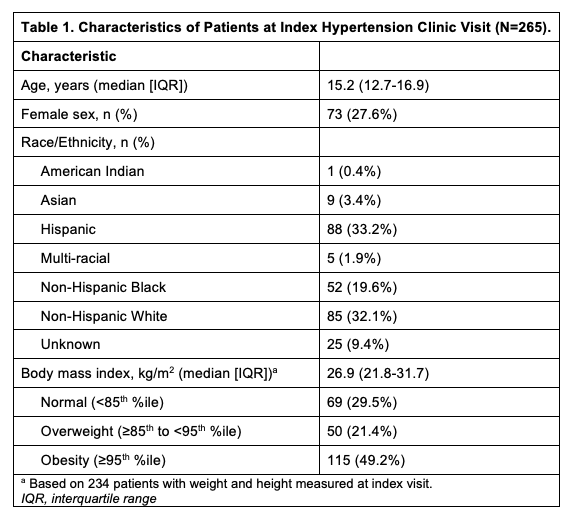
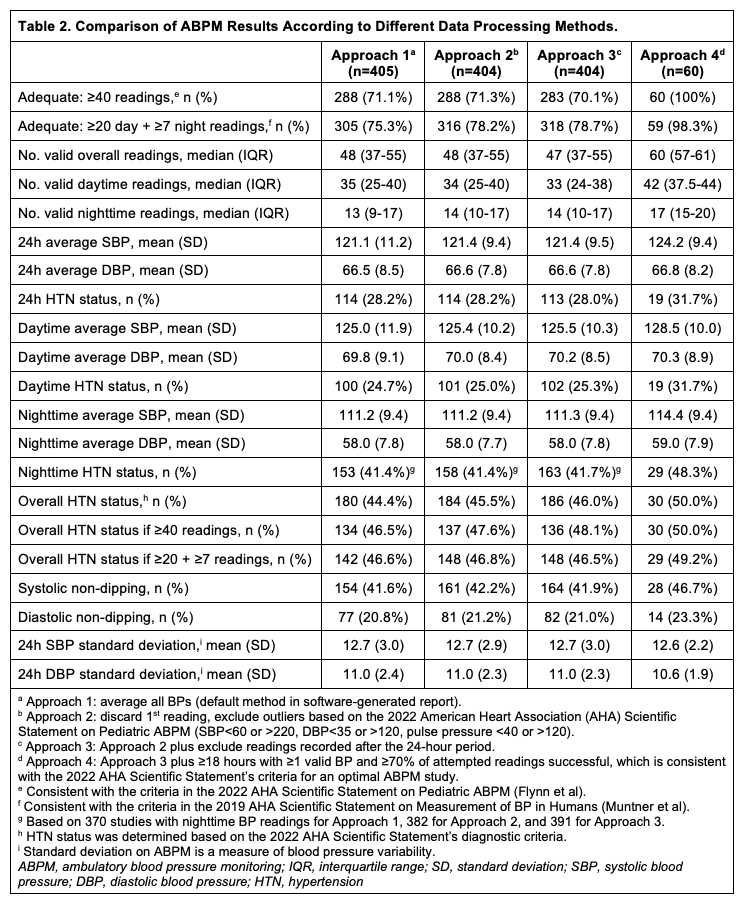
Background: Although ambulatory blood pressure monitoring (ABPM) is recommended to confirm hypertension disorder diagnosis and treatment response, implementation has been limited by technical expertise and software that provides only broad summary data. No standardized or validated methods exist to automatically collect and analyze individual-level ABPM data across diverse centers at scale. Objective: (1) Develop a pathway for the automated collection and analysis of raw patient-level ABPM data; (2) Determine how different approaches to processing ABPM data impact interpretation of ABPM results. Design/Methods: The Study of the Epidemiology of Pediatric Hypertension (SUPERHERO) is a multisite, retrospective registry of youth < 19 years evaluated in pediatric hypertension subspecialty clinics for an ICD-10 code-defined hypertension disorder from 2015-2024. A participating academic medical center in the Northeast identified patients in the SUPERHERO Registry at their site that completed ABPM. The site team downloaded raw, deidentified ABPM data, with each file named according to the patient's study ID and sleep/wake time (Fig 1). The deidentified data were shared with the data coordinating center for analysis. We compared the results of ABPM after processing the raw data using four different approaches to operationalize guideline-recommended criteria of an adequate ABPM study. Results: Of 1054 patients in SUPERHERO at the study site, 265 patients (15.2 years [IQR, 12.7-16.9], 27.6% female, 33.2% Hispanic, 32.1% white, 19.6% Black, 70.5% obesity/overweight) completed a total of 405 ABPM studies (Table 1). When defining an adequate ABPM study as ≥40 readings, the number of adequate studies was 288 (71.1%) with Approach 1 (average all BPs irrespective of timing); 288 (71.1%) with Approach 2 (discard first BP, exclude outliers, average all other BPs); 283 (69.9%) with Approach 3 (Approach 2 plus exclude BPs beyond 24h); and 60 (14.8%) with Approach 4 (Approach 3 plus ≥18h with ≥1 valid BP and ≥70% of attempted BPs successful) (Table 2). Of the 283 adequate studies in Approach 3, requiring a 70% success rate resulted in exclusion of 161 (56.9%) studies, including 156 with ≥20 daytime and ≥7 nighttime readings. The prevalence of ambulatory hypertension ranged from 44.4% in Approach 1 to 50.0% in Approach 4.
Conclusion(s): We have developed an innovation for the automated analysis of ABPM data across centers, devices, and software. Next steps will focus on analyzing ABPM data from >10,000 patients in the SUPERHERO Registry to leverage the first and largest longitudinal database of linked ABPM and electronic health record data.
Figure 1. Workflow for the Automated Collection and Analysis of Multicenter Ambulatory Blood Pressure Monitoring Data in the SUPERHERO Registry.
Table 1. Characteristics of Patients at Index Hypertension Clinic Visit (N=265).
Table 2. Comparison of ABPM Results According to Different Data Processing Methods.

 photo")