455 - Defining peripheral oxygen saturation reference ranges after birth for newborns with Congenital Diaphragmatic Hernia
Friday, April 24, 2026
5:30pm - 8:00pm ET
Publication Number: 1437.455
Anna Bostwick, Childrens Hospital of Philadelphia, Philadelphia, PA, United States; Leny Mathew, Children's Hospital of Philadelphia, Philadelphia, PA, United States; K. Taylor Wild, Children’s Hospital of Philadelphia, Philadelphia, PA, United States; Anne Ades, Childrens Hospital of Philadelphia, Philadelphia, PA, United States; Natalie Rintoul, Childrens Hospital of Philadelphia, Philadelphia, PA, United States; Tom Reynolds, Children's Hospital of Philadelphia, Philadelphia, PA, United States; Lauren Heimall, Children's Hospital of Philadelphia, Philadelphia, PA, United States; Sura Lee, Childrens Hospital of Philadelphia, Philadelphia, PA, United States; Juliana S. Gebb, Childrens Hospital of Philadelphia, Philadelphia, PA, United States; Holly L. Hedrick, Childrens Hospital of Philadelphia, Philadelphia, PA, United States; Elizabeth Foglia, Children's Hospital of Philadelphia, Swarthmore, PA, United States
Clinical Research Study Lead Childrens Hospital of Philadelphia Philadelphia, Pennsylvania, United States
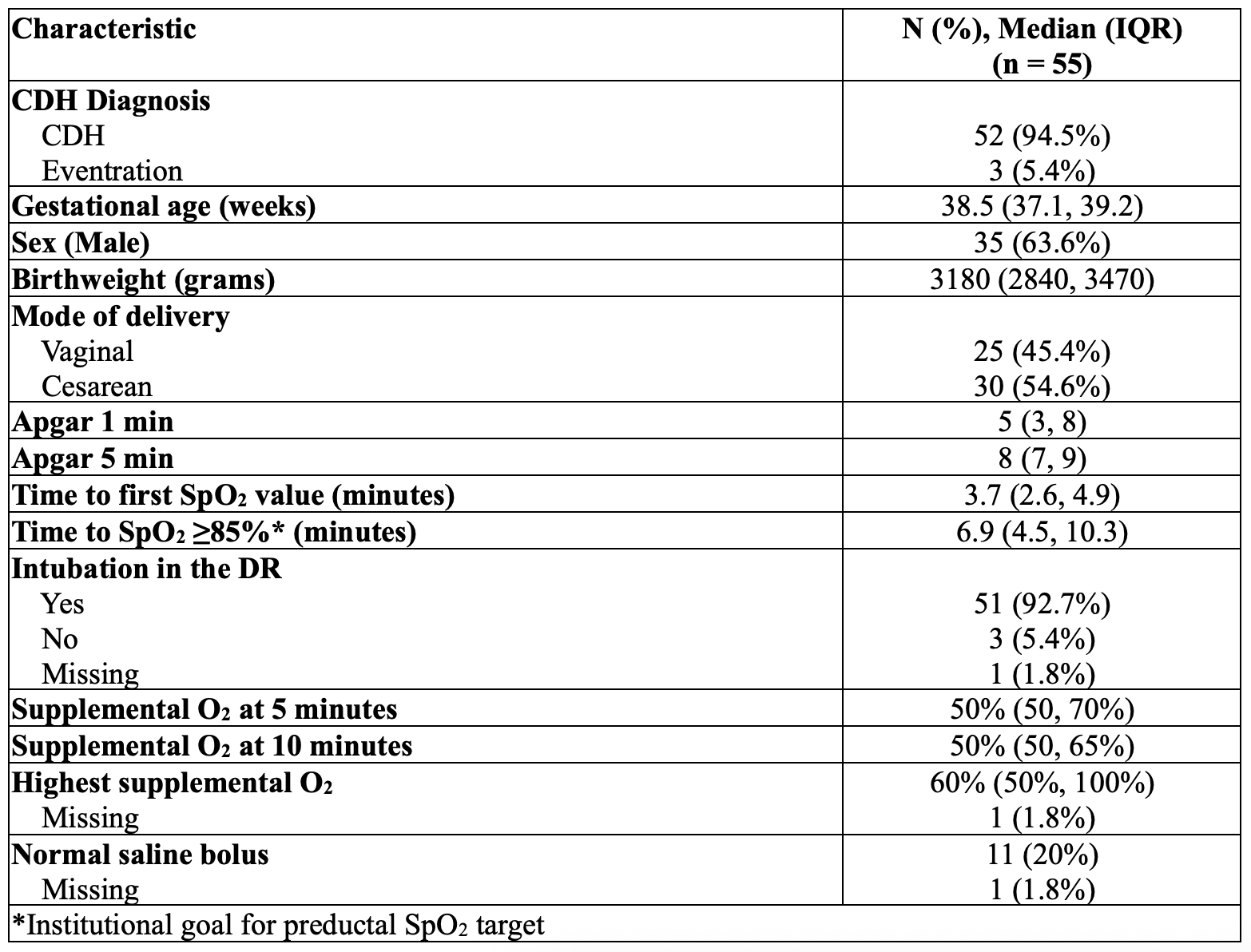
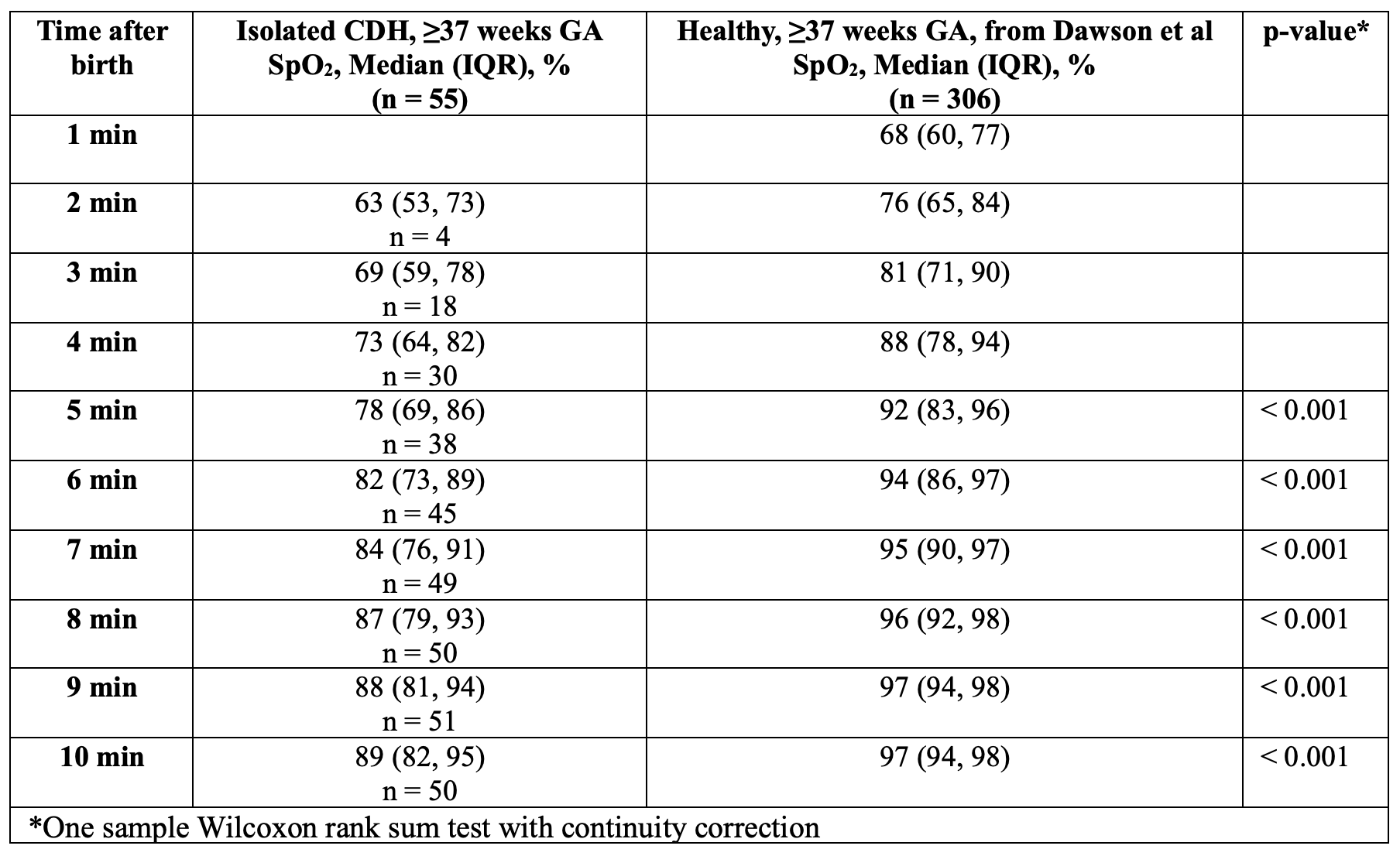
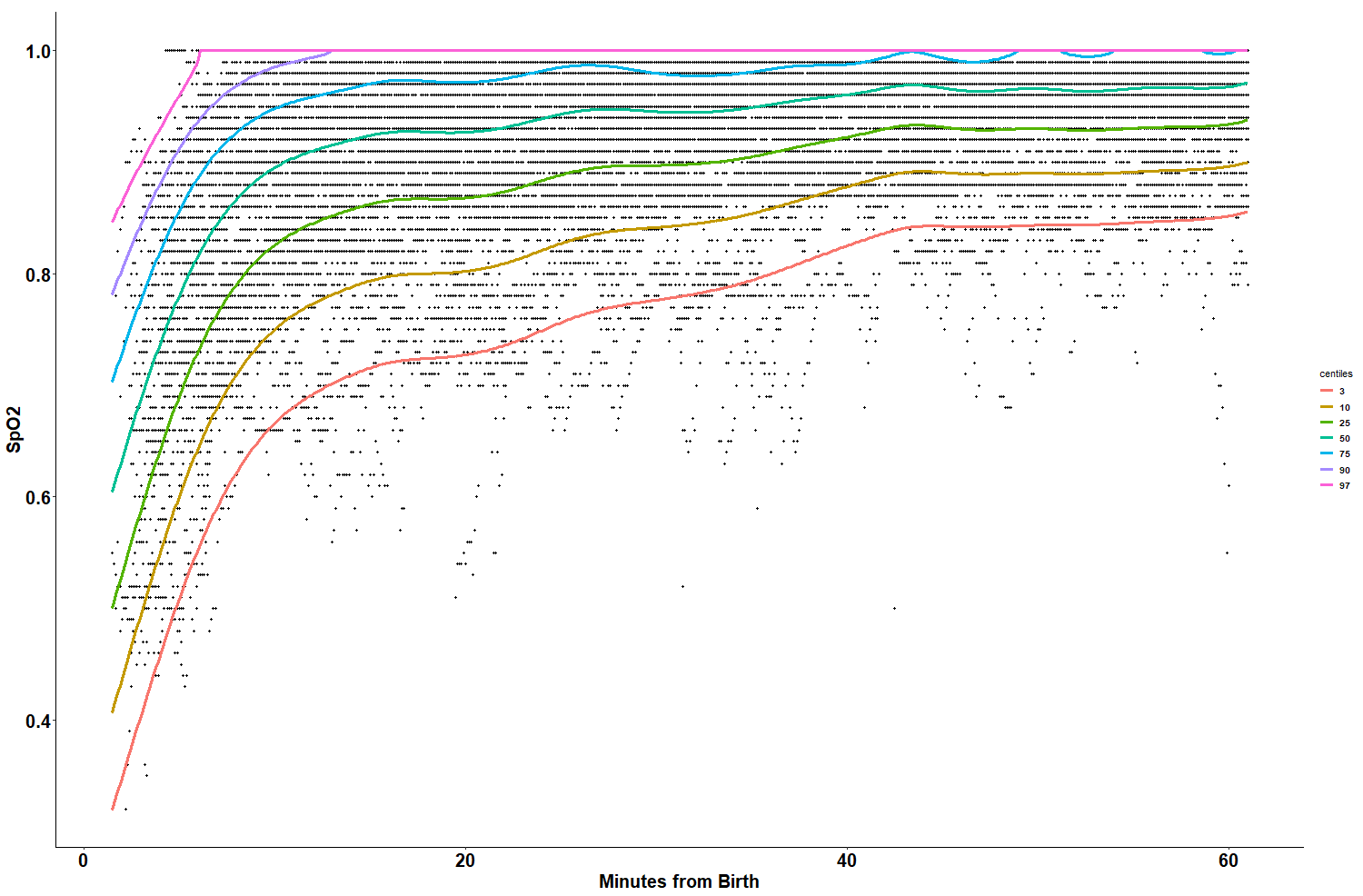
Background: Immediately after birth, newborns undergo several rapid cardiopulmonary adaptations to transition from placental to ex-utero physiology. Established nomograms for oxygen saturation (SpO2) values after birth exist for healthy newborns. Transitional cardiorespiratory physiology is inherently disrupted in many newborns with congenital anomalies such as congenital diaphragmatic hernia (CDH). The extent and nature of these differences are not well characterized. Objective: To characterize delivery room (DR) interventions and minute-to-minute SpO2 values after birth for newborns with CDH. Design/Methods: Prospective single center observational study of newborns prenatally diagnosed with isolated CDH born ≥37 weeks gestational age (GA) with physiologic monitor data recorded during the first postnatal hour. A Moberg CNS device connected to a GE Carescape recorded vital signs every 2 seconds. These data and clinical variables were collected in a clinical database. Demographics and resuscitation characteristics were summarized. One-sample Wilcoxon rank sum test was used to compare the distribution of SpO2 to established norms. The Generalized Additive Models for Location Scale and Shape (GAMLSS) was used to estimate the 3rd, 10th, 25th, 50th, 75th, 90th and 97th centiles of SpO2 up to 60 minutes after birth. Time to reach goal preductal SpO2 ≥85% was summarized. Results: In this study, 55 eligible newborns with physiologic vital sign data were born between 9/18/2022 and 1/1/2025. The median (IQR) GA was 38.5 weeks (38, 39.2), median birth weight was 3180 grams (2840, 3470), and a majority (63.6%) were male. Most patients were intubated in the DR (51 (92.7%)), and the median maximal supplemental O2 was 60% (50%, 100%) (Table 1). Median time to first SpO2 value was 3.7 minutes (2.6, 4.9). Predicted preductal SpO2 centiles are reported in Figure 1. The median SpO2 value at 5 minutes was 78% (69%, 86%) and at 10 minutes was 89% (82%, 95%), and median time to SpO2 ≥85% was 6.9 minutes with all reaching this benchmark by 48.7 minutes. The median supplemental O2 value at 5 minutes was 50% (50%, 70%) and at 10 minutes was 50% (50%, 65%).
Conclusion(s): We created centiles characterizing minute-to-minute SpO2 values during the first hour after birth for newborns with prenatally diagnosed CDH. Though all patients received resuscitation, these values are lower than published normative SpO2 values for healthy newborns. Future work should focus on the association between minute-to-minute SpO2 targets and clinical outcomes.
Table 1: Demographics and Resuscitation Characteristics
Table 2: Minute-by-minute SpO2 values for CDH compared with values published by Dawson et al
Figure 1: SpO2 centiles for the first 60 minutes after birth for isolated CDH, ≥37 weeks GA

 photo")