Session: Neonatal Pulmonology - Clinical Science 1: Bronchopulmonary Dysplasia I
366 - Significant Reduction in the Incidence of Bronchopulmonary Dysplasia After Optimization of Respiratory Care Strategy in VLBW and ELBW Infants
Friday, April 24, 2026
5:30pm - 8:00pm ET
Publication Number: 1350.366
Su Young Park, Rutgers, Robert Wood Johnson Medical School, New Brunswick, NJ, United States; Amrryn Halari, Rutgers, Robert Wood Johnson Medical School, New Brunswick, NJ, United States; Rakesh Sahni, Columbia University Vagelos College of Physicians and Surgeons, New York, NY, United States; Jen Tien T. Wung, Columbia University, Englrewood Cliffs, NJ, United States; Vadim S. Ten, Rutgers University, New Brunswick, NJ, United States
Medical Fellow Rutgers, Robert Wood Johnson Medical School New Brunswick, New Jersey, United States
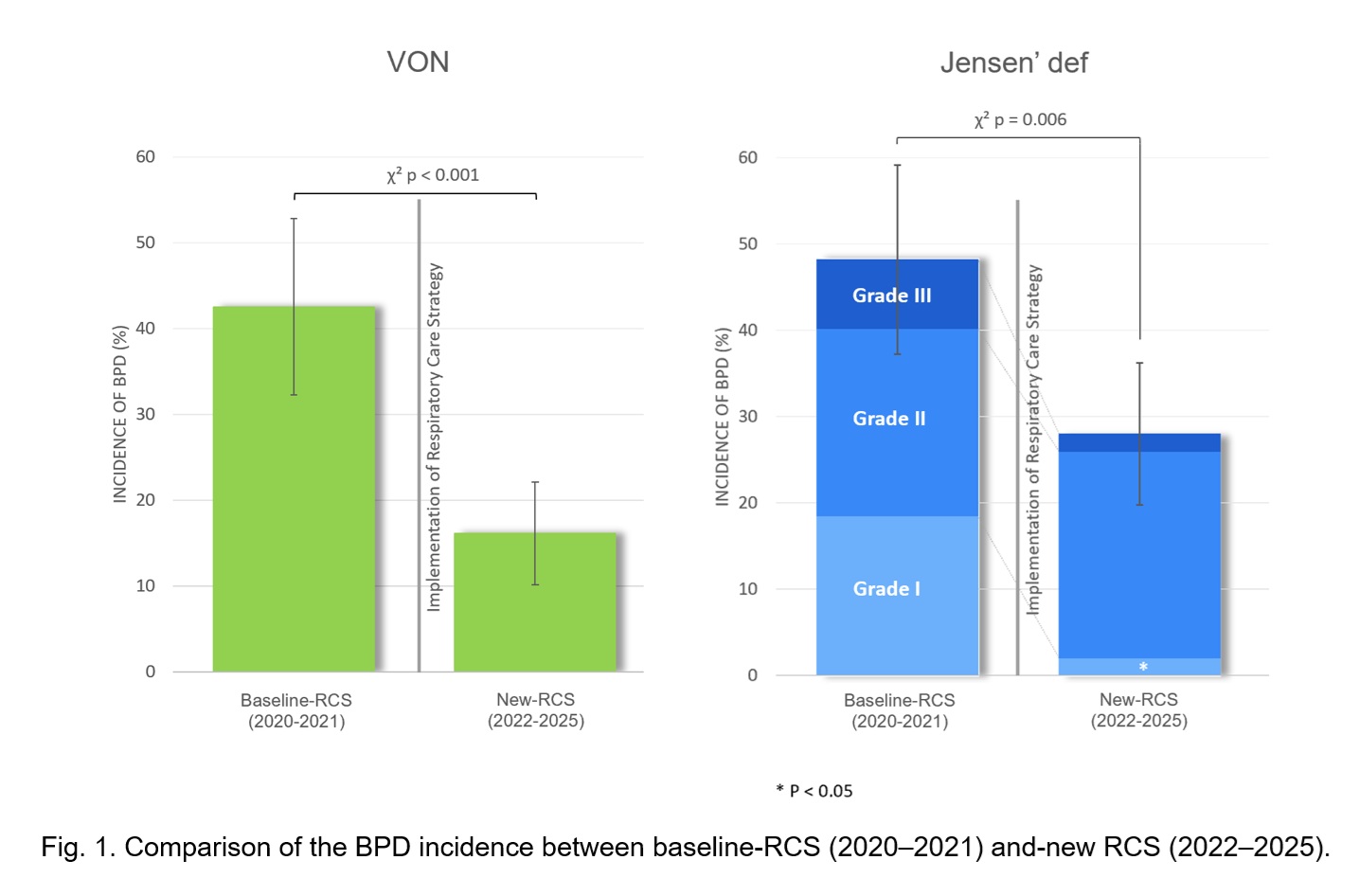
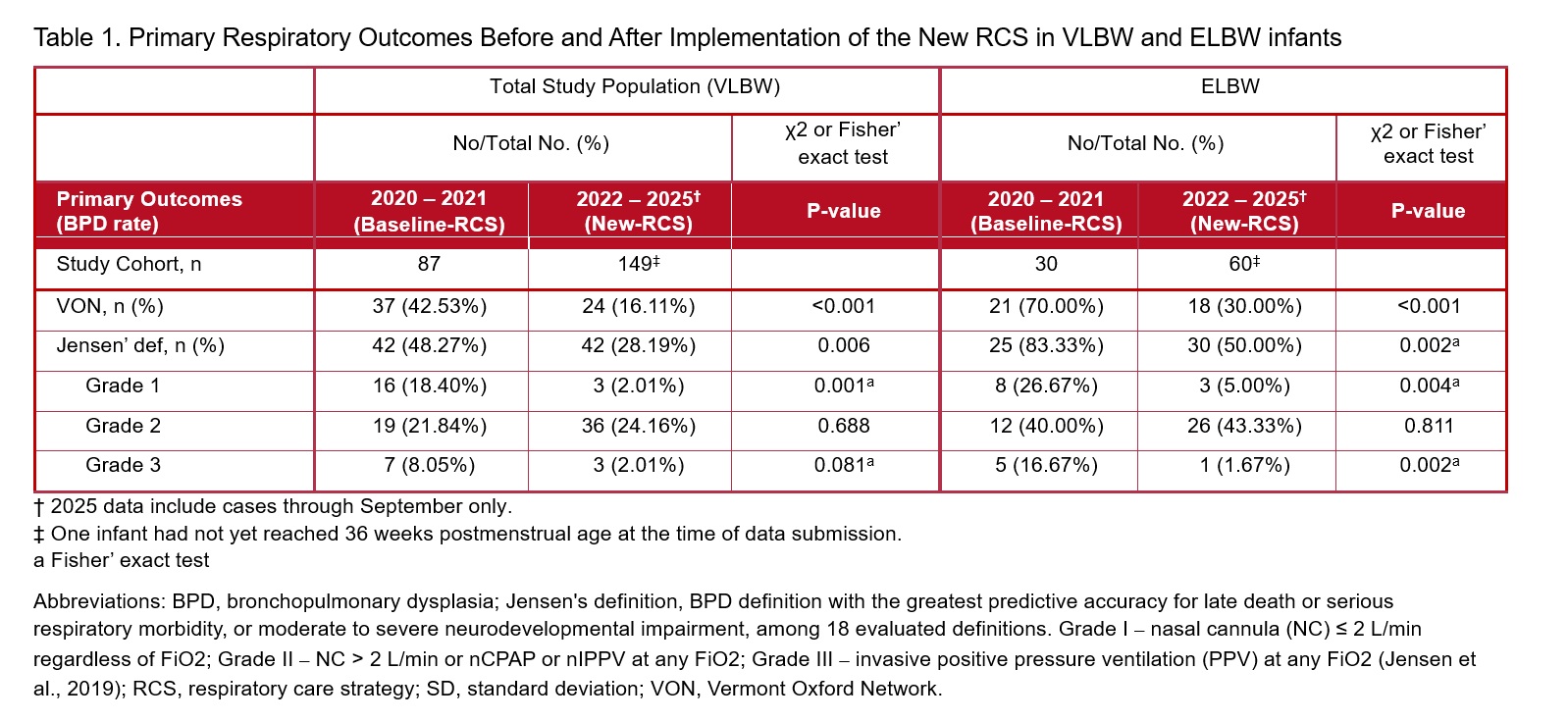
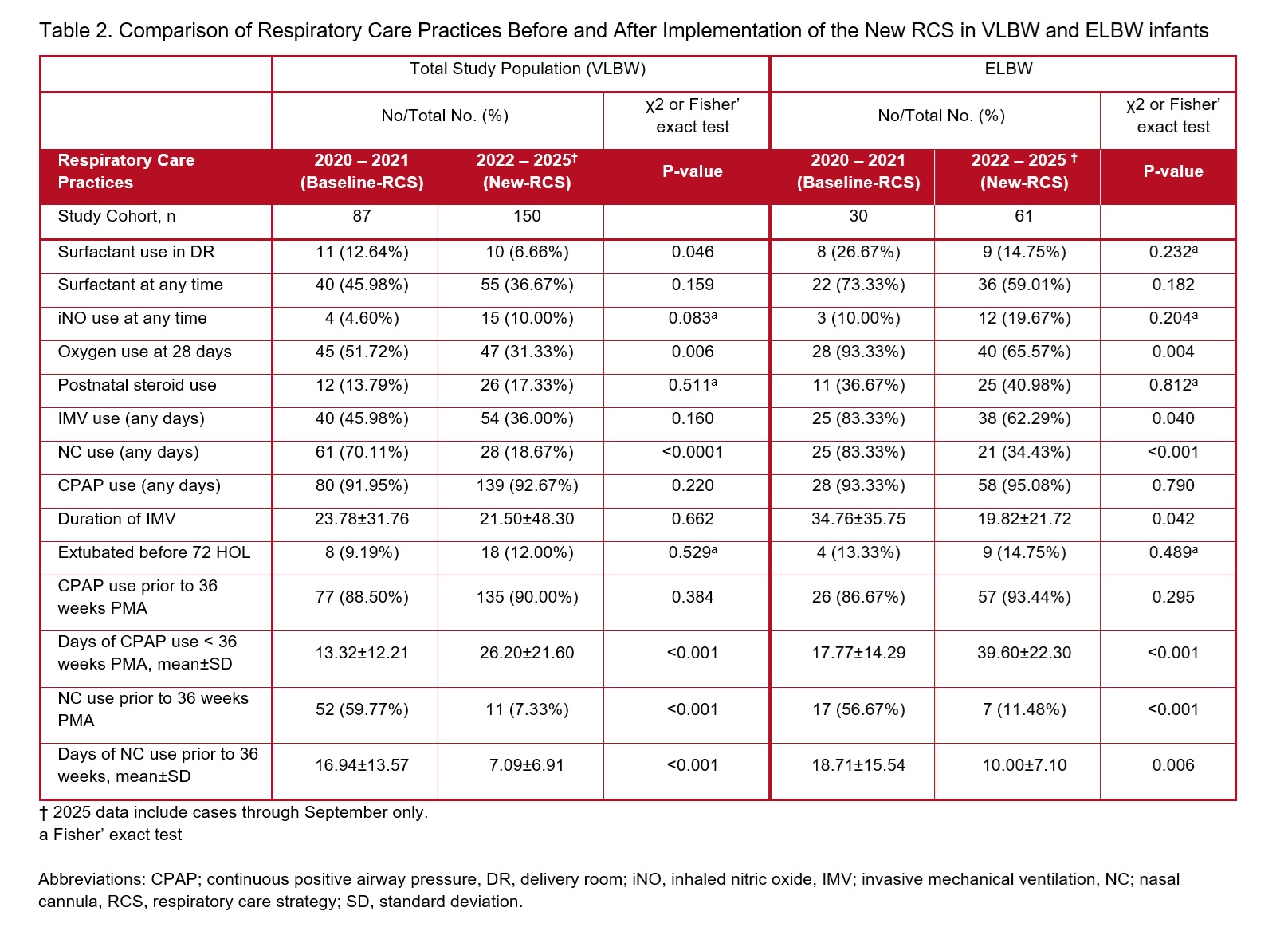
Background: Despite advances in the care of very low birth weight (VLBW) and extremely low birth weight (ELBW) infants, the incidence of bronchopulmonary dysplasia (BPD) remains high. Significant inter-center variation suggests that the BPD incidence is modifiable. Objective: We hypothesized that adopting the major principles of the respiratory care strategy (RCS) from an institution (Columbia Univ) reporting excellent respiratory outcomes can reduce BPD incidence. Design/Methods: In a retrospective chart review, we compared BPD incidence (primary outcome) before baseline-RCS (2020-21, n=87) and after implementing new RCS (2022-25, n=150). Institutional IRB approved the study. Secondary outcomes included the incidence of pneumothorax, grade III-IV IVH, cystic PVL, PDA, NEC, and ROP requiring treatment. Similar data were analyzed in ELBW infants. Compared to the baseline-RCS, the new-RCS included: (1) discontinuation of high-flow (HF) and RAM nasal cannulas use prior to 36 weeks of postmenstrual age, (2) elevation of the FiO₂ threshold for surfactant therapy from ≥0.30 to ≥0.50, and (3) use of bubble nasal CPAP (5-6 cm H₂O) as the primary mode of respiratory support in spontaneously breathing infants. BPD was defined using Vermont Oxford Network (VON) criteria and the definition with the greatest predictive accuracy for late death or serious respiratory and neurodevelopmental morbidity by Jensen et al [1]. Outcomes were analyzed using χ² or Fisher' exact test. Results: Demographics (GA, BW, gender, Apgar score, etc) and mortality did not differ. After implementing new RCS, BPD incidence declined from 42.5% to 16.1%, p< 0.001 (VON), and from 48.3% to 28.2%, p=0.006 (Jensen). In ELBW infants, the BPD incidence also decreased, from 70.0% to 30.0%, p< 0.001 (VON), and from 83.3% to 50.0%, p=0.002 (Jensen), (Fig.1, Tab.1). New RCS significantly decreased the use of oxygen at 28 days of life, need for surfactant therapy, the use of high and low flow nasal cannulas, increased the use of CPAP, and decreased days on ventilator in ELBW infants (Tab.2). No differences were found in secondary outcomes.
Conclusion(s): Implementing three key components: avoiding the use of early HF and RAM cannulas, raising FiO₂ thresholds for surfactant therapy, and use of bubble CPAP as the primary mode of respiratory care was associated with a significant reduction in the BPD incidence without affecting other morbidities. These findings support the feasibility of implementing better practices from one center to another and call for a multicenter trial to confirm reproducibility. [1] Jensen EA et al. Am J Respir Crit Care Med. 2019;200(6):751-759
Figure1. Comparison of the BPD incidence between baseline-RCS (2020-2021) and new-RCS (2022-2025).
Table 1. Primary Respiratory Outcomes Before and After Implementation of the New RCS in VLBW and ELBW infants.
Table 2. Comparison of Respiratory Care Practices Before and After Implementation of the New RCS in VLBW and ELBW infants.