396 - Hypoargininmia and Hypocitrullinemia in Bronchopulmonary dysplasia associated pulmonary hypertension in preterm infants
Friday, April 24, 2026
5:30pm - 8:00pm ET
Publication Number: 1379.396
Abdallah Alkhaldi, University of Texas Medical Branch School of Medicine, Galveston, TX, United States; Areeba makhdoom, UT Houston, Friendswood, TX, United States; Sunil K. Jain, University of Texas Medical Branch, Galveston, TX, United States
Resident University of Texas Medical Branch School of Medicine Galveston, Texas, United States
Background: About one-third of premature infants with bronchopulmonary dysplasia (BPD) develop BPD-associated pulmonary hypertension (BPD-PH). In preterm infants, reduced nitric oxide bioavailability due to oxidative stress, inflammation, and decreased arginine (ARG) and citrulline (CIT) levels may promote pulmonary vascular remodeling leading to BPD-PH. We aimed to assess the relationship between plasma ARG and CIT concentrations at 36 weeks corrected gestational age (CGA), BPD severity, and BPD-PH. Objective: To determine whether plasma ARG and CIT levels at 36 weeks CGA are associated with BPD severity and the presence of BPD-PH in preterm infants < 30 weeks' gestation. Design/Methods: In this prospective observational study, preterm infants < 30 weeks admitted to the UTMB NICU (July 2022-July 2025) were included. Infants with major heart or chromosomal anomalies or who did not survive to 36 weeks CGA were excluded. Screening echocardiography at 36 weeks CGA evaluated for BPD-PH, defined by septal flattening or systolic eccentricity index ≥ 1.15. Plasma ARG and CIT were quantified by liquid chromatography-mass spectrometry. One-way ANOVA compared ARG and CIT across BPD grades (1-3), and the Mann-Whitney U test compared infants with BPD-PH versus BPD alone (p < 0.05). Results: Fifty-nine infants ( < 30 weeks) were studied; 34 (58%) were male, mean gestational age 27.2 ± 1.4 weeks, mean birth weight 940 ± 210 g. Thirteen (22%) had grade 1 BPD, 28 (47%) grade 2, and 18 (31%) grade 3. Mean (± SD) ARG levels were 66.9 ± 54.3, 56.3 ± 67.4, and 51.6 ± 66.3 µmol/L; CIT 417.1 ± 327.7, 395.3 ± 415.9, and 79.9 ± 94.1 µmol/L, respectively, decreasing with greater BPD severity. Infants with BPD-PH had lower ARG (82.5 ± 93.2 vs 117.1 ± 153.5 µmol/L) and CIT (529.4 ± 438.8 vs 625.2 ± 556.7 µmol/L; p < 0.05).
Conclusion(s): Lower plasma ARG and CIT concentrations were associated with higher BPD severity and BPD-PH in preterm infants, suggesting impaired nitric-oxide precursor availability may contribute to pulmonary vascular disease in BPD and warrants validation in larger multicenter cohorts.
Figure 1. Mean plasma citrulline and arginine concentrations by BPD grade
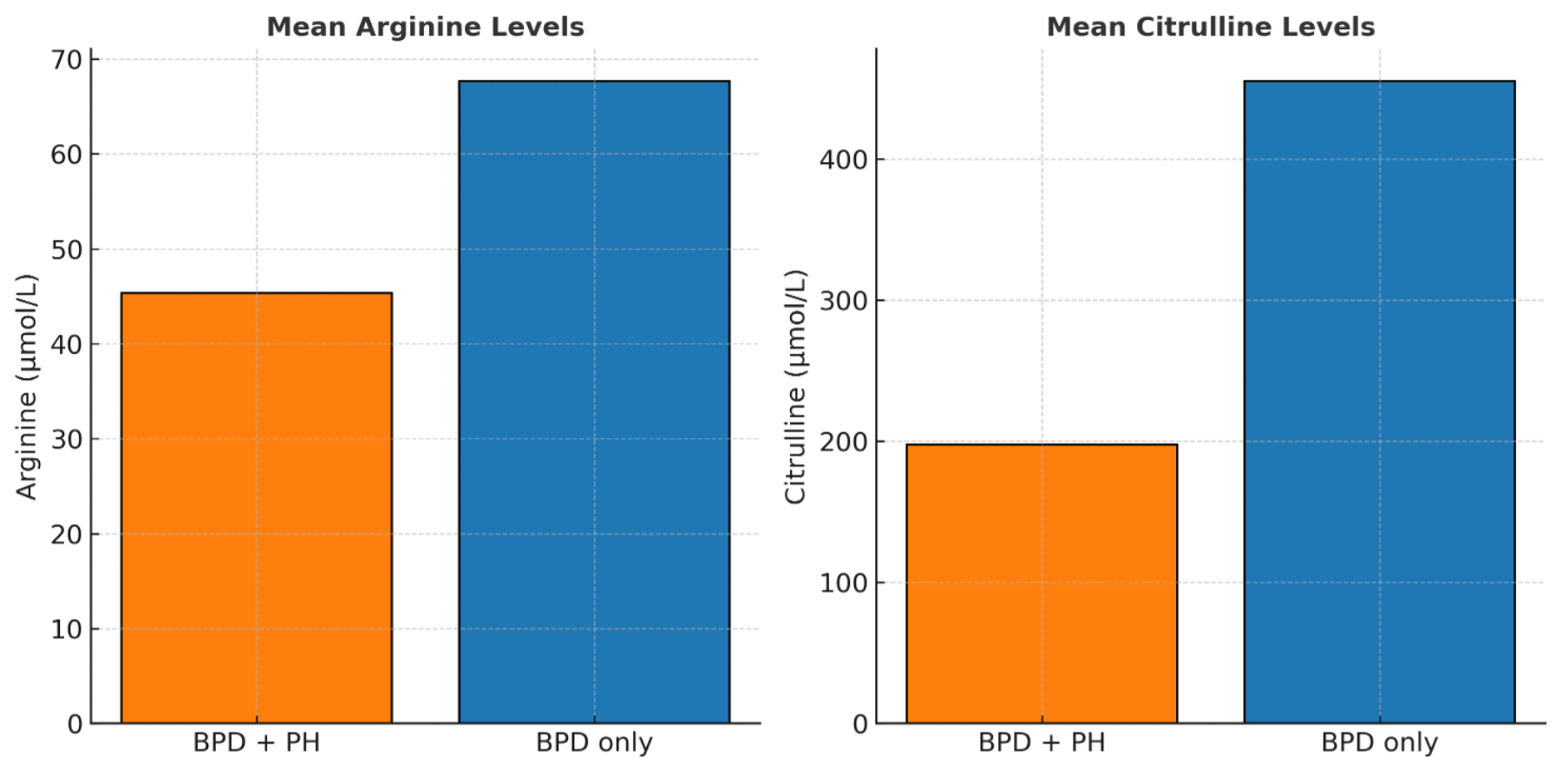
Figure 2. Mean plasma arginine and citrulline concentrations in infants with BPD-associated pulmonary hypertension (BPD-PH) compared with BPD alone


.png)