761 - Reconfiguring Neonatal Intensive Care Unit (NICU) Discharge Planning Processes To Promote Early Discharges In A Level III-C NICU
Friday, April 24, 2026
5:30pm - 8:00pm ET
Publication Number: 1737.761
Amruta Bamanikar, Hackensack Meridian School of Medicine, Short hills, NJ, United States; Nina S. Solanki, K. Hovnanian Children's Hospital at Jersey Shore University Medical Center, Holmdel, NJ, United States; Elizabeth J. Assing, Hackensack Meridian School of Medicine, Manasquan, NJ, United States; Amanda Woodford, K. Hovnanian Children's Hospital at Jersey Shore University Medical Center, Neptune, NJ, United States; Kaitlyn Philips, Joseph M. Sanzari Children's Hospital Hackensack University Medical Center, North Caldwell, NJ, United States; Vitaliya Boyar, K. Hovnanian Children's Hospital at Jersey Shore University Medical Center, middletown, NJ, United States
Physician Hackensack Meridian School of Medicine Short hills, New Jersey, United States
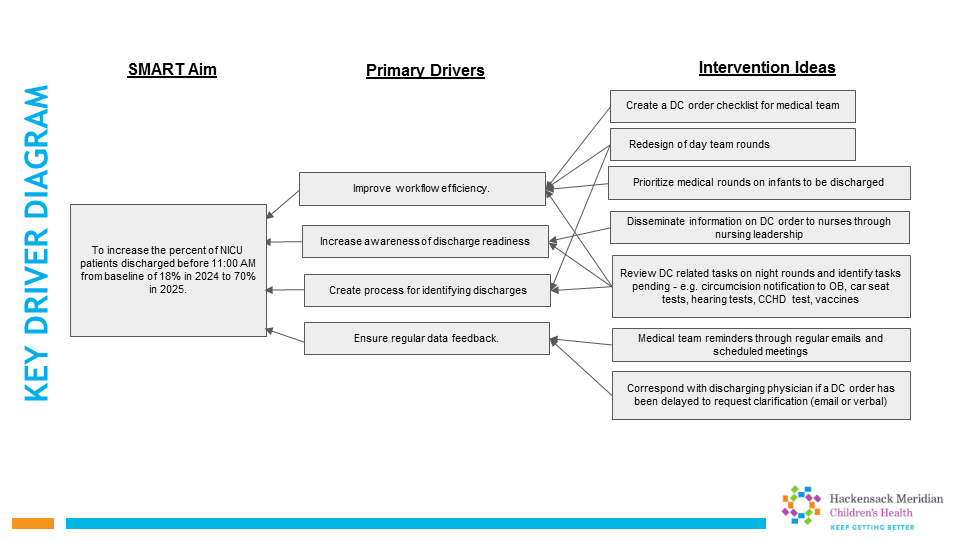
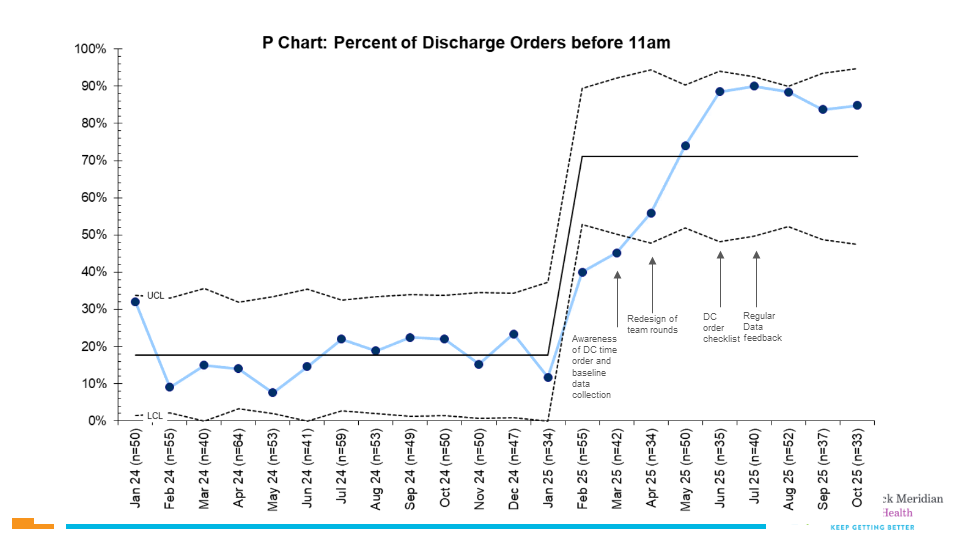
Background: Hospitals prioritize early discharges to facilitate bed availability and optimize resource and staff utilization. In the Neonatal Intensive Care Unit (NICU), one key intervention is for providers to enter discharge orders (DC order) by a certain time. In order to enter the DC order in a timely manner, several crucial and interconnecting tasks across different services need to be completed. In 2024, a quality review of the discharges from our NICU found that we had less than 50% of discharge orders placed before 11:00am. Objective: To increase the percent of NICU patients with a DC order entered before 11am from 18% in 2024 to 70% in 2025. Design/Methods: This QI project took place in a level III NICU at an academic, integrated children's hospital. We used the Model for Improvement as our framework for instituting change. A multidisciplinary team collaborated to observe and understand the current discharge process. We used a Fishbone diagram (Fig 1) to identify themes related to delayed discharge, then organized the project's approach in a key driver diagram (Fig 2). Interventions included: creation of three simultaneous rounding teams, identification of anticipated discharges on unit huddle board, incorporating review of discharge tasks on night rounds, priority rounding, discharge order checklist, weekly emails to discharging physicians if DC order was delayed, monthly reminders and data sharing. The primary outcome "DC order" was defined as the percent of patients discharged before 11am, excluding mortalities and transfers out. The process measure was emails sent to physicians regarding delayed discharges. The balancing measure was readmissions within 7 days of discharges and perceived concerns of expediting discharge related-tasks from caregivers and/or the medical team. DC order was plotted on a p-chart and analyzed for special cause variation. Results: The percent of early DC orders increased from 18% in 2024 to 80% in 2025 (Fig 3). Simultaneous rounding teams, ongoing awareness and nursing engagement were key to success. There were no readmissions nor concerns from caregivers or the medical team with the early discharge process. We identified family factors as the biggest contributor to delayed discharges from the NICU once the DC order was placed: specifically, caregiver presence in the NICU. Our next steps are to aim for a 2-hour interval from DC order to actual discharges.
Conclusion(s): Our project to increase early DC orders was successful. Our next initiative is to investigate factors associated with caregiver presence in the NICU on day of discharge.
Fishbone Diagram Contributors to Late Discharge (DC) Orders
Key Driver Diagram to Increase NICU Discharge Orders before 11:00AM

 Credit")
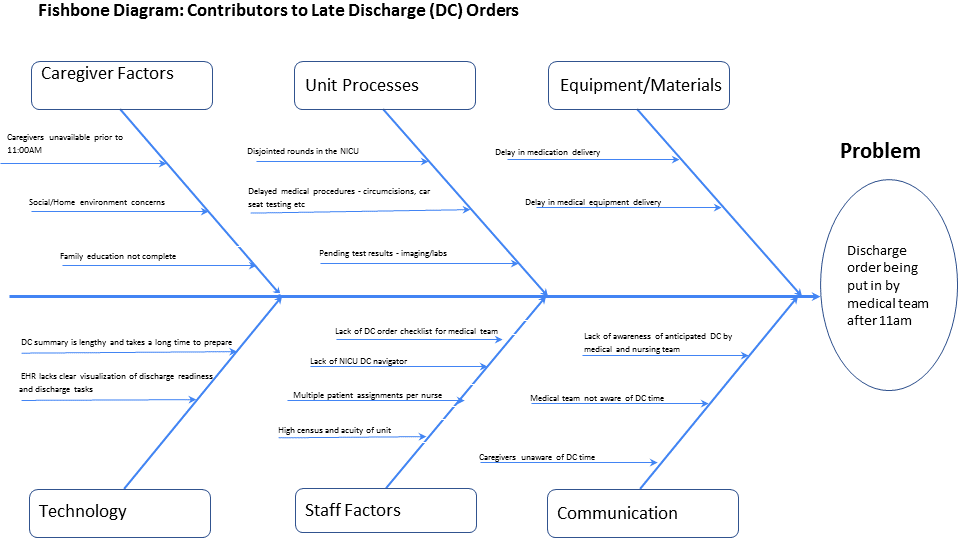 Contributors to Late Discharge (DC) Orders
Contributors to Late Discharge (DC) Orders