420 - Accuracy and Acceptability of Nocturnal Home Blood Pressure Monitoring Versus Ambulatory Blood Pressure Monitoring in Youth: A Mixed Methods Study
Friday, April 24, 2026
5:30pm - 8:00pm ET
Publication Number: 1403.420
James T. Nugent, Yale School of Medicine, New Haven, CT, United States; Victoria Cueto Vilorio, Yale School of Medicine, New Haven, CT, United States; Hugh M. Medvecky, The Warren Alpert Medical School of Brown University, Guilford, CT, United States; Geisa Wilkins, Yale School of Medicine, New Haven, CT, United States; Emily B. Finn, Yale School of Medicine, New Haven, CT, United States; Tammy Brady, Johns Hopkins Children's Center, Baltimore, MD, United States; Jason H. Greenberg, Yale School of Medicine, New Haven, CT, United States; Mona Sharifi, Yale School of Medicine, New Haven, CT, United States
Assistant Professor of Pediatrics Yale School of Medicine New Haven, Connecticut, United States
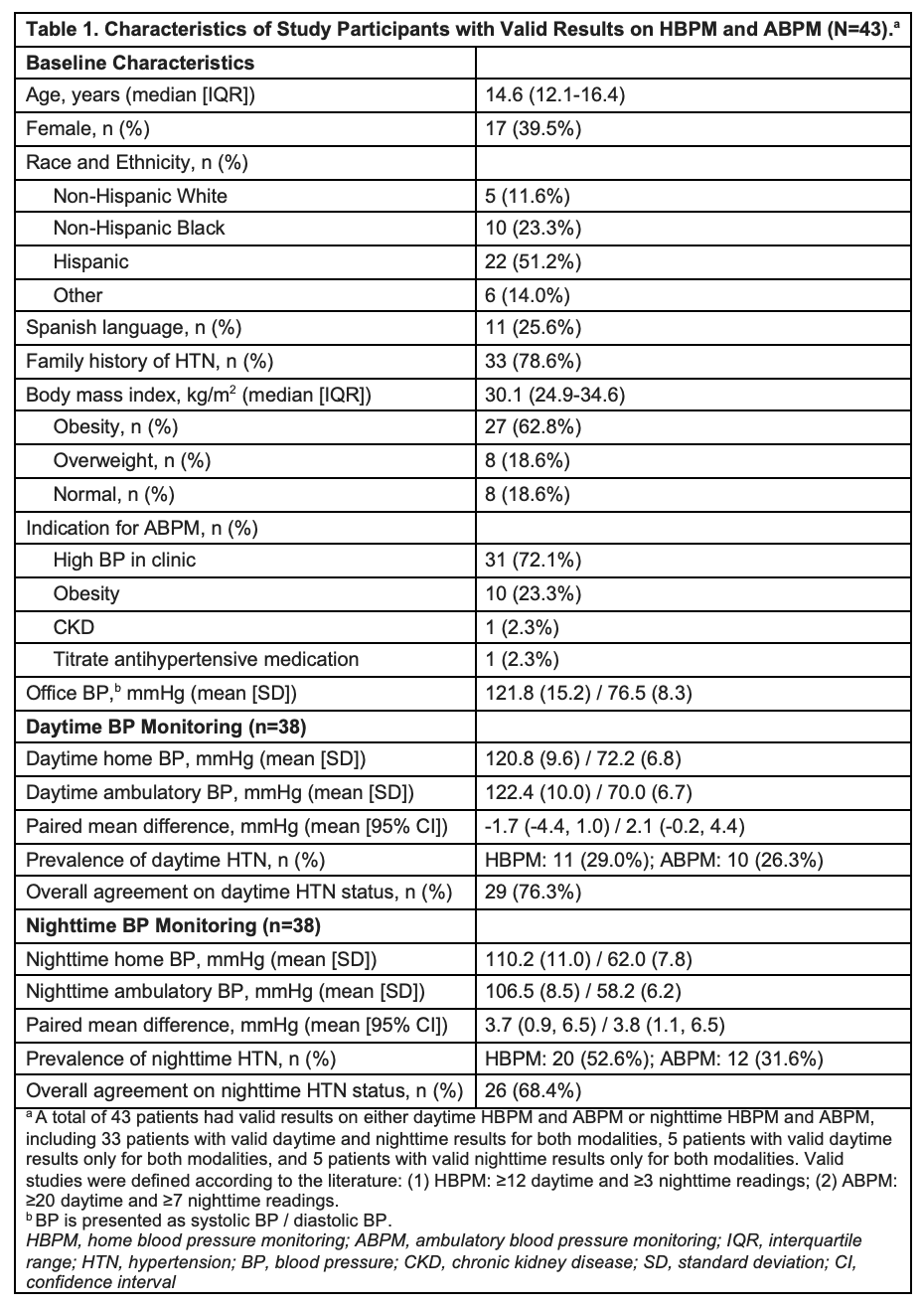
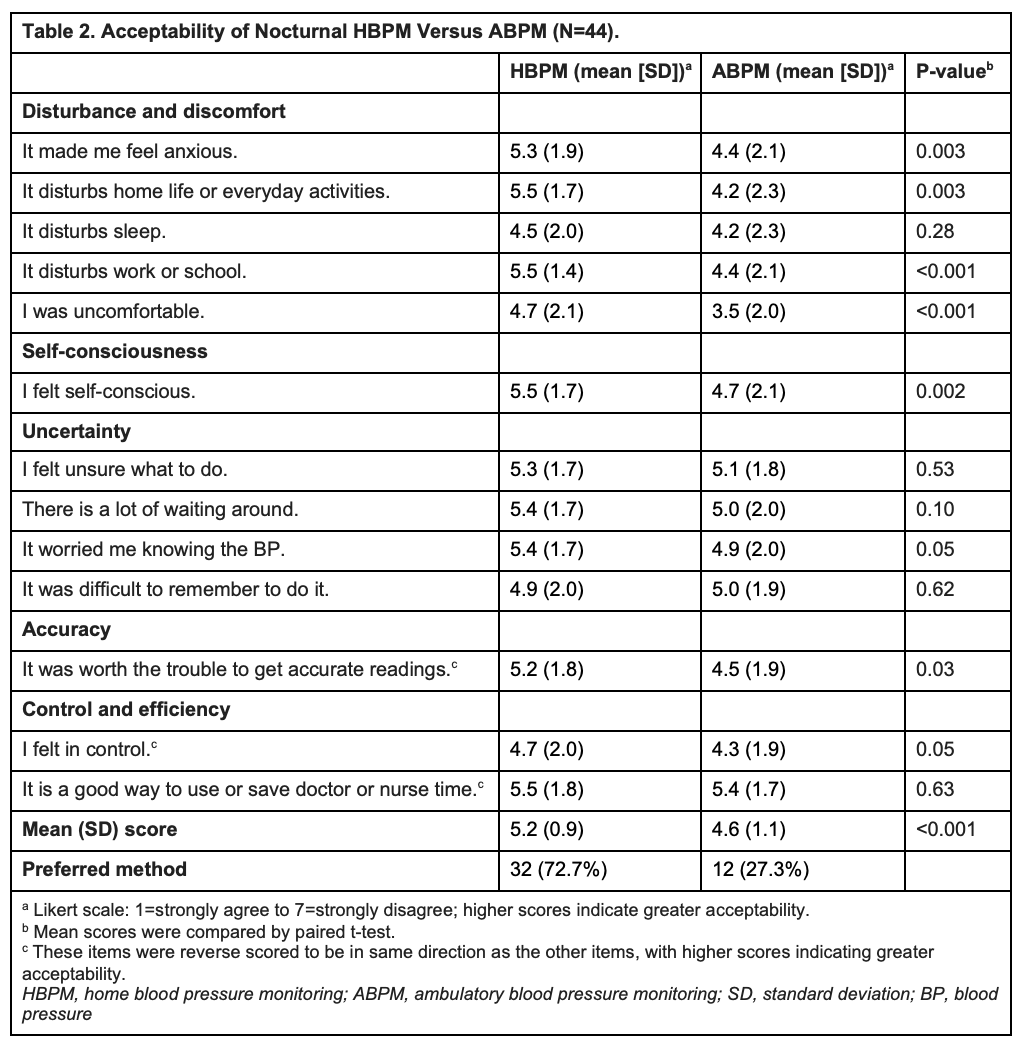
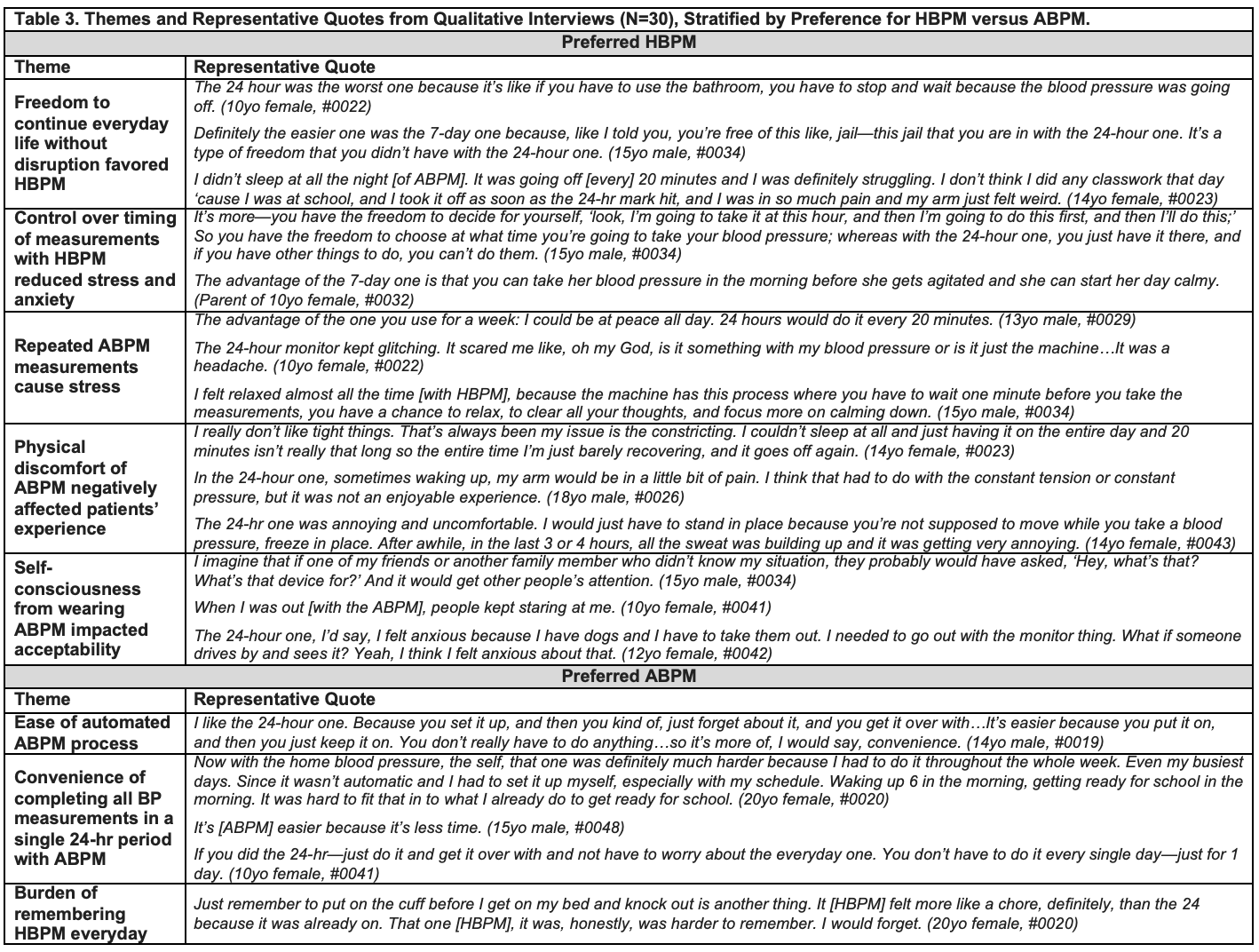
Background: Although adult guidelines allow for home blood pressure monitoring (HBPM) as an alternative to ambulatory blood pressure monitoring (ABPM), there is insufficient evidence to support the same recommendation in pediatrics. Objective: Evaluate the accuracy and acceptability of HBPM compared with ABPM in youth. Design/Methods: We conducted a prospective, mixed methods study of youth 6-21y with an indication for ABPM recruited from pediatric hypertension (HTN) and primary care clinics at a Northeast medical center from 2023-2025. Participants completed 24h ABPM (SpaceLabs 90227) and HBPM (Microlife WatchBP Home N upper arm device) within a 4wk period. For HBPM, participants took duplicate morning and evening BPs x7d and overnight HBPM x3 nights (3 hourly BPs/night). Participants were invited to complete a validated survey to calculate an overall acceptability score (range 1-7) for each device and a semistructured qualitative interview guided by the Unified Theory of Acceptance and Use of Technology 2 with transcripts analyzed using thematic analysis. Results: Of 54 participants with ambulatory and home BP readings, 43 participants (14.6y [IQR, 12.1-16.4], 40% female, 51% Hispanic, 81% obesity/overweight) had adequate readings on both modalities (Tbl 1). Daytime HBPM was similar to ABPM (systolic/diastolic mean difference, -1.7 [95% CI, -4.4, 1.0]/2.1 [-0.2, 4.4], P=0.22/0.07). Nighttime HBPM was higher than ABPM (3.7 [0.9, 6.5]/3.8 [1.1, 6.5], P=0.01/0.008). Agreement for HTN classification was 76% for daytime and 68% for nighttime. Overall mean (SD) acceptability score was higher for HBPM (5.2 [0.9]) than ABPM (4.6 [1.1]) (P < 0.001), with the largest differences for items related to disturbance and discomfort (Tbl 2). Most participants preferred HBPM (73% vs 27%). We achieved thematic saturation after 30 interviews. Participants who preferred HBPM emphasized control ("you choose where you measure it, when you want to measure it"); freedom to continue activities ("you're free of this jail that you are in with the 24h one"); physical discomfort from ABPM ("constant tension"); and self-consciousness with ABPM ("people kept staring at me") (Tbl 3). Participants who preferred ABPM valued the ease of the fully automated process ("you set it up and forget about it") and disliked the burden of daily HBPM ("the home monitor felt like a chore").
Conclusion(s): HBPM and ABPM were closely associated and had modest agreement in HTN classification. HBPM was preferred by most participants, though some found daily HBPM difficult. These results can inform shared decision-making on the patient-centered selection of BP modalities.
Table 1. Characteristics of Study Participants with Valid Results on HBPM and ABPM (N=43).
Table 2. Acceptability of Nocturnal HBPM Versus ABPM (N=44).
Table 3. Themes and Representative Quotes from Qualitative Interviews (N=30), Stratified by Preference for HBPM versus ABPM.

 photo")