38 - Impact of Genetic Disorders on Outcomes of Infants Who Underwent Therapeutic Hypothermia for Neonatal Encephalopathy
Friday, April 24, 2026
5:30pm - 8:00pm ET
Publication Number: 1031.38
Marina Metzler, Washington University in St. Louis School of Medicine, ST LOUIS, MO, United States; Isabella Zaniletti, IZ Statistics LLC, Tampa, FL, United States; Karna Murthy, Ann & Robert H. Lurie Children's Hospital of Chicago, Chicago, IL, United States; Jennifer A. Rumpel, University of Arkansas for Medical Sciences College of Medicine, Little Rock, AR, United States; Michael A.. Padula, Childrens Hospital of Philadelphia, Philadelphia, PA, United States; Theresa Grover, University of Colorado School of Medicine, Aurora, CO, United States; Rakesh Rao, Washington University in St. Louis School of Medicine, St. Louis, MO, United States; Jennifer A. Wambach, Washington University School of Medicine/St. Louis Children's Hospital, Saint Louis, MO, United States
Fellow Washington University in St. Louis School of Medicine ST LOUIS, Missouri, United States
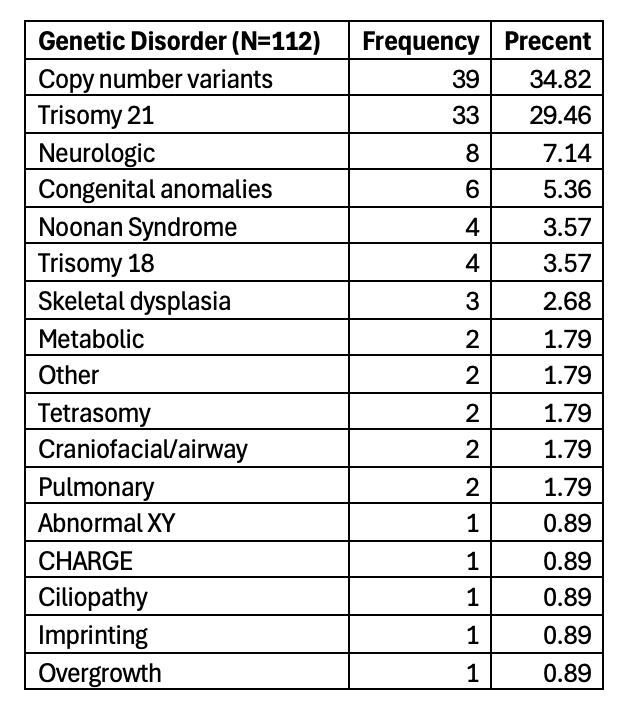
Background: Genetic disorders and neonatal encephalopathy secondary to suspected hypoxic-ischemic encephalopathy (HIE) are common causes of morbidity and mortality in NICU infants. Most infants with HIE treated with therapeutic hypothermia (TH) do not have precipitating sentinel events. Infants with underlying genetic disorders (GD) may present with features that overlap with or mimic HIE. Identifying infants with a genetic disorder earlier may alter treatment and reduce exposure to TH and potential complications. However, there is paucity of evidence describing the burden of genetic disorders in this population. Objective: To determine if infants with HIE/GD could be distinguished a priori from infants with HIE treated with TH. Design/Methods: We performed a retrospective study of infants hospitalized from January 2017 to May 2025 using the Children's Hospitals Neonatal Consortium (CHNC) database. We included infants greater than or equal to 35 weeks gestation who underwent TH. We excluded infants if TH was initiated after 7 hours of life or with post-arrest/non-perinatal TH. We identified genetic diagnoses based manual review. Data were analyzed using Chi-Square and Wilcoxon Rank Sum tests. Results: Of the 5,437 infants included, 5,351 (98.4%) infants had HIE and 86 (1.6%) had HIE and a genetic diagnosis (HIE/GD). Chromosome anomalies (35%) and Trisomy 21 (29%) were the most common genetic diagnoses (Table 1).
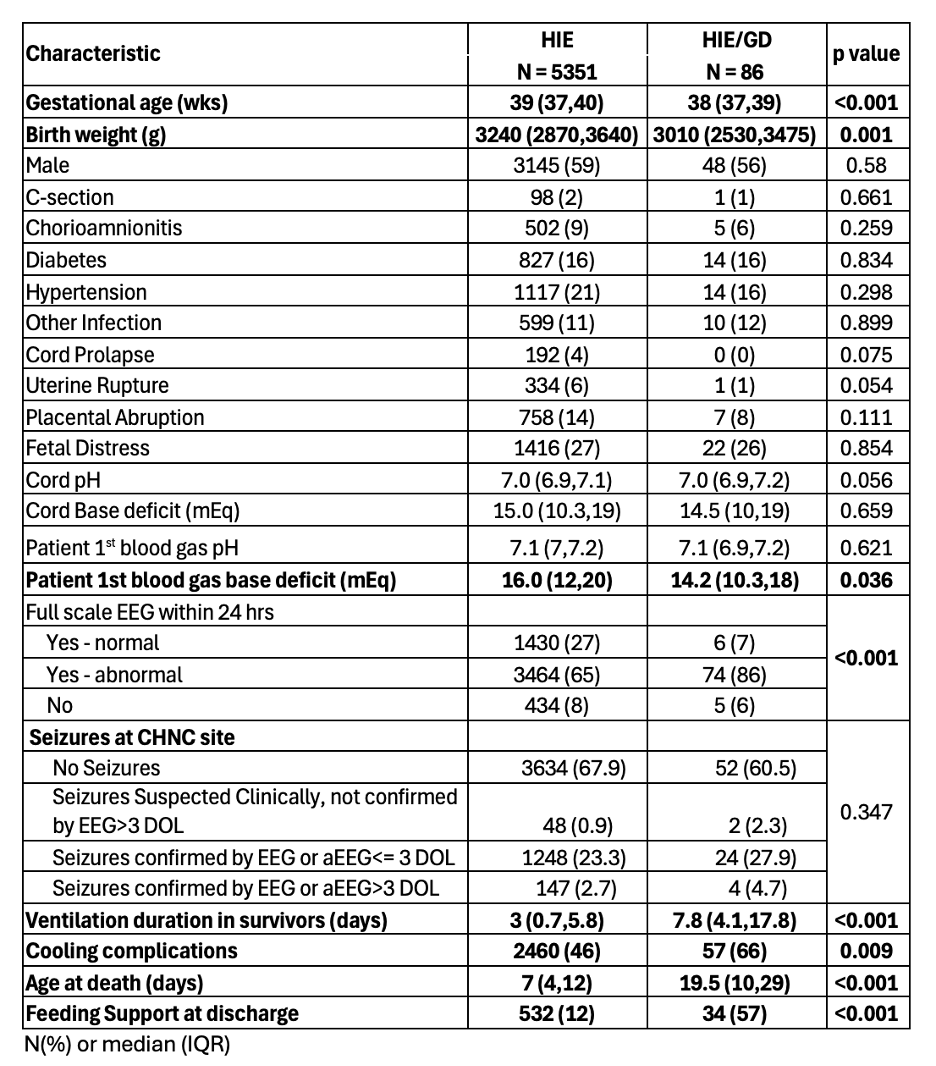
Infants with HIE/GD were born earlier, had lower birth weight and were less acidotic at presentation (Table 2). Seizures did not differ, while EEG background was more likely to be abnormal in infants with HIE/GD. Infants with HIE/GD were also ventilated longer, had longer lengths of stay and died later compared to infants with HIE (Table 2). HIE/GD were also more likely to have complications from cooling (p=0.009) and need feeding support at discharge (G-tube or NG, p< 0.0001).
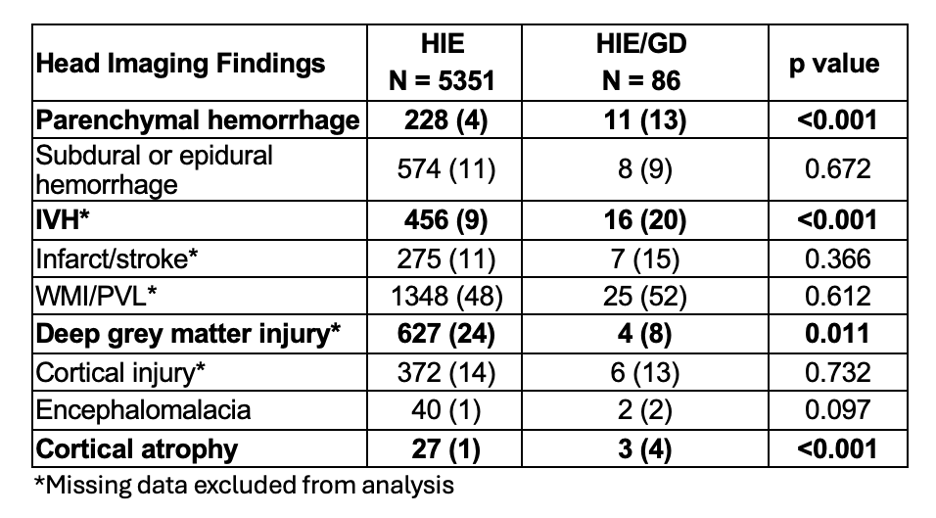
On head imaging, parenchymal or intraventricular hemorrhage and cortical atrophy were more common in HIE/GD, while deep grey matter injury was more frequent in the HIE group (Table 3).
Conclusion(s): Overall, 1.6% of infants who underwent TH were identified to have a genetic diagnosis. HIE/GD infants were born earlier and could not be distinguished by perinatal or birth characteristics, however, were associated with higher morbidities and differed in neuroimaging characteristics. Identification of an underlying GD in this cohort remains challenging, but may impact prognostication, management, and counseling for risk recurrence.

 photo")