585 - Expedited patient evaluation by Pediatric Emergency Medicine Fellow Physicians in triage to improve care.
Friday, April 24, 2026
5:30pm - 8:00pm ET
Publication Number: 1562.585
Nguyen D. Nguyen, University of Texas Southwestern Medical School, Dallas, TX, United States; Jacob Phouthavong-Murphy, UT Southwestern Medical Center, Dallas, TX, United States; Brian Wagers, University of Texas Southwestern Medical School, Lewisville, TX, United States; Angie Rodick, Children's Health, Dallas, TX, United States; Macy B. Ackermann, Children's Health, Allen, TX, United States; Jennifer Vaughan, Children's Health, Keller, TX, United States; Jo-Ann O. Nesiama, University of Texas Southwestern Medical School, Dallas, TX, United States
Clinical Fellow University of Texas Southwestern Medical School Dallas, Texas, United States
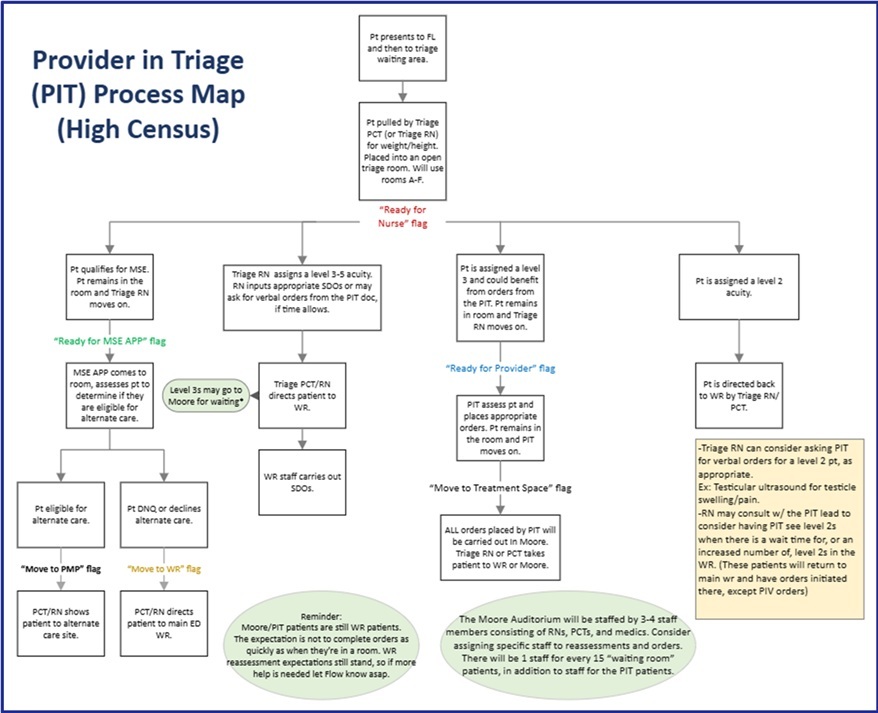
Background: Multiple studies have demonstrated that licensed independent providers (LIPs) in triage decrease Emergency Department (ED) wait times, improve throughput and door-to-provider times, and add efficiency to patient care. However, there is little literature that addresses whether trainee physicians in triage can achieve similar benefits. Objective: Our objectives were to (1) decrease the number of Emergency Severity Index (ESI) 2 and 3 patients who left without being seen (LWBS) in the ED utilizing Pediatric Emergency Medicine (PEM) Fellows in triage, (2) evaluate the effect of overall ED length of stay (LOS) on all patients, when the provider in triage (PIT) process was being utilized, and (3) assess fellow experience and satisfaction. Design/Methods: A PEM fellow was stationed in triage from 3PM to 11PM to evaluate patients with an ESI score of 2 or 3 between November 3, 2024, to April 26, 2025, as this is considered peak times of patient volumes. Any ordered lab work or imaging was started prior to assignment of an ED bed. Pre- and post-implementation metrics were obtained and compared including total patient volumes, total time in ED room (TT:ED), and number of patients left without being seen (LWBS). Additionally, a 5-question survey was sent to the participating PEM fellows to determine experience and satisfaction. Results: Pre- and post-implementation patient volumes were similar, 32,478 and 33,936, respectively. Patients who LWBS prior to implementation were highest between 6PM and 2AM with an overall average of 2.9%. After implementation, there was a decrease in the number of patients who LWBS to 1.6%, with the largest decreases observed during the same time frame. Total time in ED room for all patients was observed to decrease by a total of 206,834 minutes throughout the 6-month implementation period. This saved time allowed for the evaluation and management of an additional 786 patients. Fellows' response to the survey was 80% (8/10) with all reporting greater autonomy and improved medical decision-making, leading to an overall enhanced fellowship experience.
Conclusion(s): Implementation of strategies to reduce ED throughput time and expedite evaluation can be used effectively in a tertiary medical center. PEM fellow physicians, who are not independent LIPs, can provide an initial assessment with the goal of reducing ED throughput time and number of patients who LWBS. Moreover, this strategy has proven to enhance fellows' training and satisfaction.

.jpg)
.jpg)
