
Neonatal Pulmonology
Session: Neonatal Pulmonology - Clinical Science 2: Bronchopulmonary Dysplasia II

Timothy Nelin, MD, MSHP
Attending Physician
Childrens Hospital of Philadelphia
Philadelphia, Pennsylvania, United States
.png) Abbreviations: BPD, bronchopulmonary dysplasia; SVI, social vulnerability index; pH, hydrogen ion concentration; pCO2, partial pressure of carbon dioxide; WBC, white blood cell.
Abbreviations: BPD, bronchopulmonary dysplasia; SVI, social vulnerability index; pH, hydrogen ion concentration; pCO2, partial pressure of carbon dioxide; WBC, white blood cell.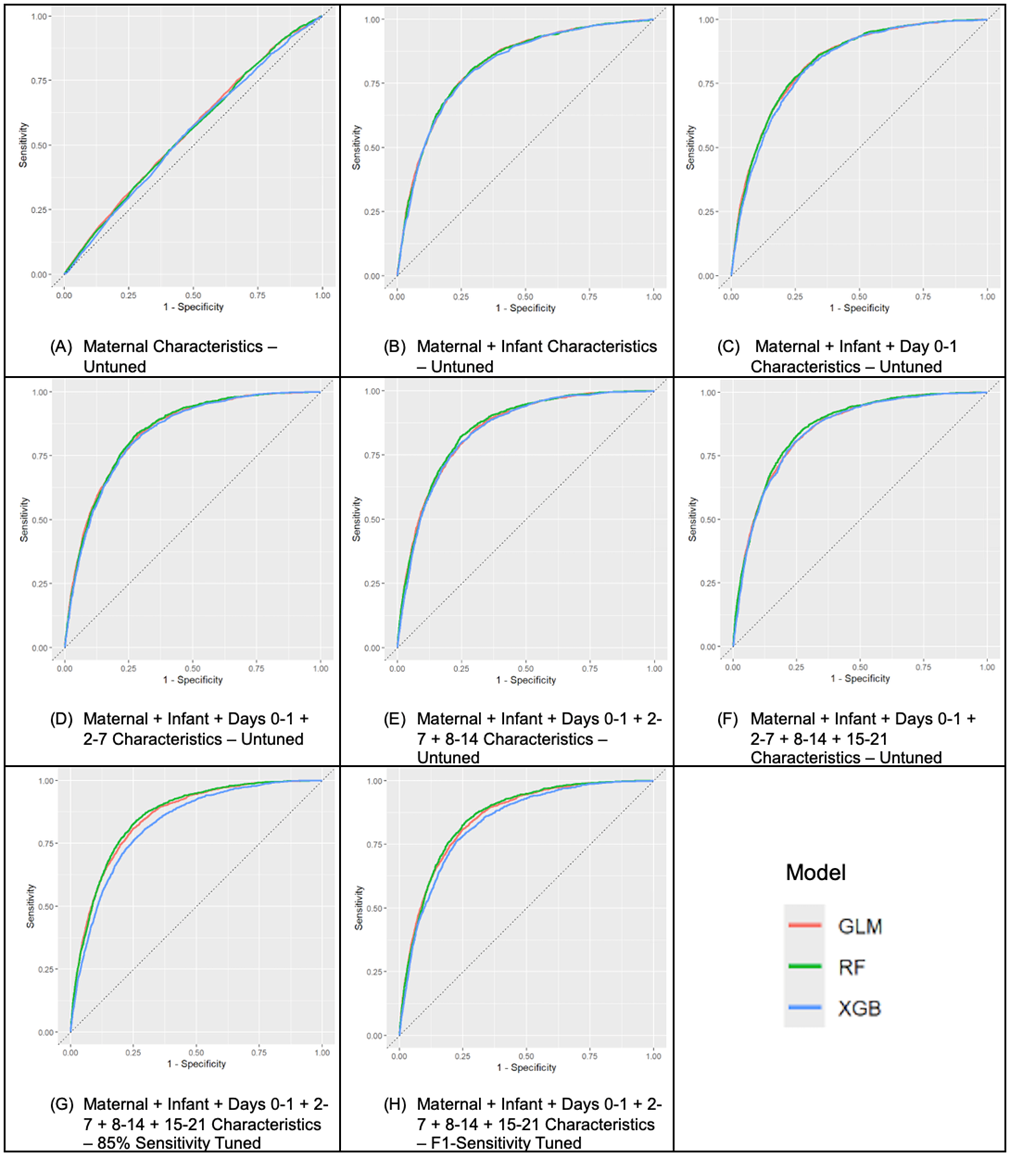 Panels A-F show untuned models incorporating progressively more data: (A) maternal characteristics; (B) maternal + infant birth characteristics; (C-F) addition of clinical data from days 0-1, 2-7, 8-14, and 15-21. Panels G and H display tuned models at 15-21 days using 85% sensitivity and F1-threshold strategies. Logistic regression (GLM), random forest (RF), and XGBoost (XGB) models were compared at each step. Discrimination improved after adding birth characteristics (AUC 0.50 to 0.82) and plateaued thereafter (AUC 0.83-0.86 across 0-21 days). At 15-21 days, positive predictive values (PPV) remained modest (0.23-0.60) given the outcome prevalence of 11.8%, while negative predictive values (NPV) were high across all models (0.91-0.98). Untuned models demonstrated high overall accuracy (0.90-0.91) but poor sensitivity (GLM 0.17, RF 0.02, XGB 0.14). The untuned RF model achieved AUC 0.86, accuracy 0.90, sensitivity 0.02, specificity 0.99, positive predictive value (PPV) 0.60, and negative predictive value (NPV) 0.91. The F1-tuned model provided balanced performance (AUC 0.86, accuracy 0.84, sensitivity 0.67, specificity 0.85, PPV 0.33, NPV 0.96), while the 85%-sensitivity-tuned model increased case detection (AUC 0.86, accuracy 0.74, sensitivity 0.85, specificity 0.72, PPV 0.25, NPV 0.98). The plateau in AUC after birth data underscores the dominant influence of perinatal characteristics despite the addition of physiologic variables.
Panels A-F show untuned models incorporating progressively more data: (A) maternal characteristics; (B) maternal + infant birth characteristics; (C-F) addition of clinical data from days 0-1, 2-7, 8-14, and 15-21. Panels G and H display tuned models at 15-21 days using 85% sensitivity and F1-threshold strategies. Logistic regression (GLM), random forest (RF), and XGBoost (XGB) models were compared at each step. Discrimination improved after adding birth characteristics (AUC 0.50 to 0.82) and plateaued thereafter (AUC 0.83-0.86 across 0-21 days). At 15-21 days, positive predictive values (PPV) remained modest (0.23-0.60) given the outcome prevalence of 11.8%, while negative predictive values (NPV) were high across all models (0.91-0.98). Untuned models demonstrated high overall accuracy (0.90-0.91) but poor sensitivity (GLM 0.17, RF 0.02, XGB 0.14). The untuned RF model achieved AUC 0.86, accuracy 0.90, sensitivity 0.02, specificity 0.99, positive predictive value (PPV) 0.60, and negative predictive value (NPV) 0.91. The F1-tuned model provided balanced performance (AUC 0.86, accuracy 0.84, sensitivity 0.67, specificity 0.85, PPV 0.33, NPV 0.96), while the 85%-sensitivity-tuned model increased case detection (AUC 0.86, accuracy 0.74, sensitivity 0.85, specificity 0.72, PPV 0.25, NPV 0.98). The plateau in AUC after birth data underscores the dominant influence of perinatal characteristics despite the addition of physiologic variables.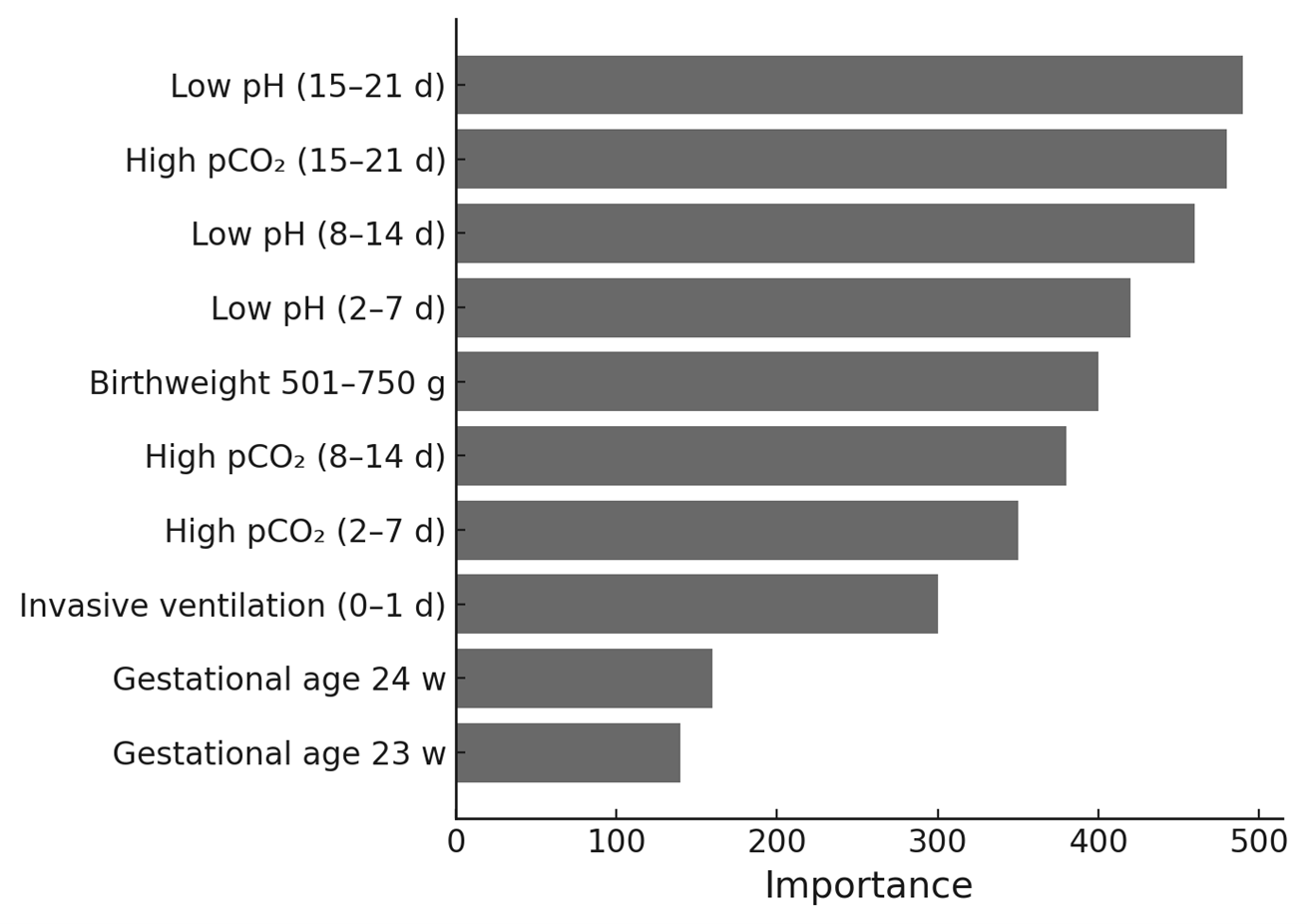 Permutation-based out-of-bag (OOB) importance estimates identify the most influential predictors in the final 15-21-day random forest model. Maternal, perinatal, and early postnatal variables were: maternal age, race and ethnicity, insurance type, rural-urban classification, social vulnerability index, smoking, antenatal steroid exposure, gestational hypertension, gestational diabetes, pre-existing hypertension, obesity, and diabetes; gestational age, birth weight category, sex, and small-for-gestational-age status; and serial physiologic and laboratory indicators of clinical status across days 0-1, 2-7, 8-14, and 15-21 of life - specifically low pH, high pCO2, abnormal white blood cell count ( <5 or >35 × 109/L), and exposure to invasive ventilation. The ten variables with highest permutation importance were low pH (15-21 days), high pCO2 (15-21 days), low pH (8-14 days), low pH (2-7 days), birth weight 501-750 g, high pCO2 (8-14 days), high pCO2 (2-7 days), invasive ventilation (0-1 days), gestational age 24 weeks, and gestational age 23 weeks. Collectively, these findings underscore the roles of persistent respiratory acidosis and extreme prematurity in predicting severe BPD or death despite broad inclusion of maternal and perinatal factors.
Permutation-based out-of-bag (OOB) importance estimates identify the most influential predictors in the final 15-21-day random forest model. Maternal, perinatal, and early postnatal variables were: maternal age, race and ethnicity, insurance type, rural-urban classification, social vulnerability index, smoking, antenatal steroid exposure, gestational hypertension, gestational diabetes, pre-existing hypertension, obesity, and diabetes; gestational age, birth weight category, sex, and small-for-gestational-age status; and serial physiologic and laboratory indicators of clinical status across days 0-1, 2-7, 8-14, and 15-21 of life - specifically low pH, high pCO2, abnormal white blood cell count ( <5 or >35 × 109/L), and exposure to invasive ventilation. The ten variables with highest permutation importance were low pH (15-21 days), high pCO2 (15-21 days), low pH (8-14 days), low pH (2-7 days), birth weight 501-750 g, high pCO2 (8-14 days), high pCO2 (2-7 days), invasive ventilation (0-1 days), gestational age 24 weeks, and gestational age 23 weeks. Collectively, these findings underscore the roles of persistent respiratory acidosis and extreme prematurity in predicting severe BPD or death despite broad inclusion of maternal and perinatal factors.