689 - Prediction Model for Necrotizing Enterocolitis-Attributable Mortality in Preterm Infants with Surgical Necrotizing Enterocolitis
Friday, April 24, 2026
5:30pm - 8:00pm ET
Publication Number: 1666.689
Dwayne Mascarenhas, The Hospital for Sick Children, Toronto, ON, Canada; Ujjwala Mantha, University of Toronto Temerty Faculty of Medicine, Toronto, ON, Canada; Shravan Kanaparthi, The Hospital for Sick Children, Toronto, ON, Canada; Jordan Mann, The Hospital for Sick Children, Toronto, ON, Canada; Nandkishor S. Kabra, Surya Hospitals Mumbai, Mumbai, Maharashtra, India; Bonny Jasani, The Hospital for Sick Children, Toronto, ON, Canada
Staff Physician & Assistant Professor Mount Sinai Hospital, Toronto Toronto, Ontario, Canada
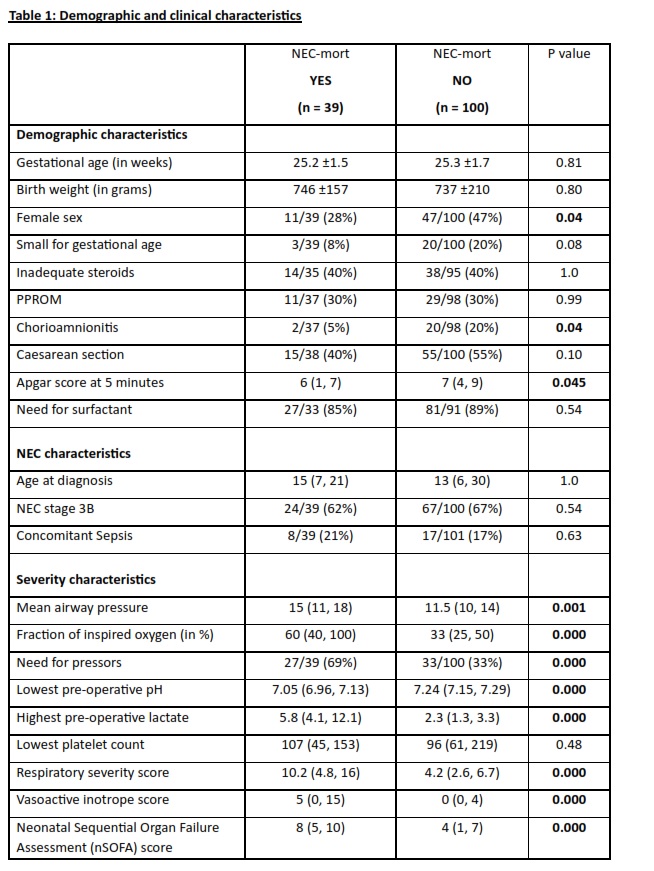
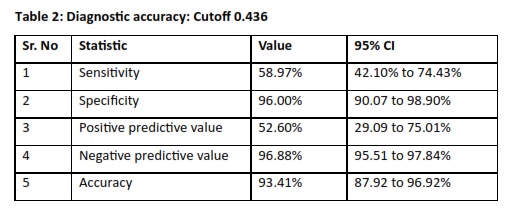
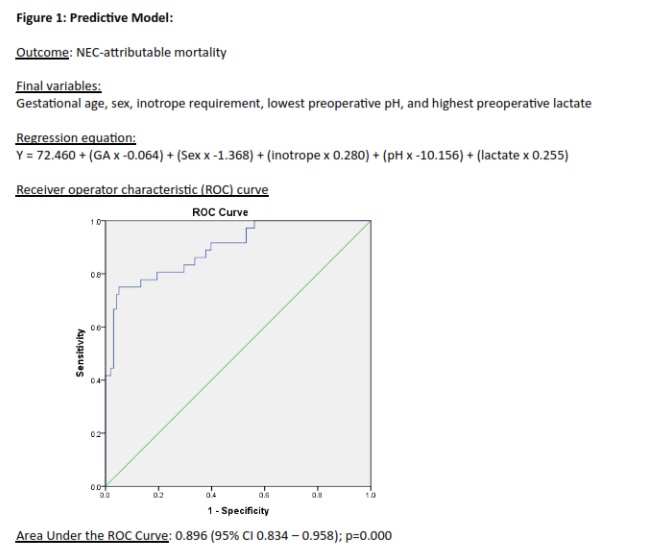
Background: Surgical necrotizing enterocolitis (sNEC) is a leading cause of mortality in preterm infants. A predictive model for NEC-attributable mortality is needed to enable early risk stratification and guide timely interventions. Objective: To develop a predictive model for NEC-attributable mortality in preterm infants with sNEC. Design/Methods: This retrospective cohort study included preterm infants ≤30 weeks with sNEC at a single quaternary neonatal intensive care unit between January 1, 2016 and June 30, 2024. Clinical and laboratory variables prior to surgery were extracted to identify predictors of NEC-attributable mortality. Multivariable logistic regression was used to develop the predictive model. The model performance was assessed using area under the receiver operating characteristic curve (AUC) and am optimal cutoff score was determined using Youden's index. Diagnostic accuracy metrics were calculated, and model co-efficients were used to construct a bedside risk prediction tool. Results: A total of 139 preterm infants with sNEC were included (mean gestational age 25.2 ±1.6 weeks, birth weight 740 ±196 grams), with 28% mortality attributable to NEC. Non-survivors had significantly higher mean airway pressures, fraction of inspired oxygen, greater need for inotropes, lower pH, and higher lactate levels. The final multivariable model identified gestational age, sex, need for inotropes, lowest preoperative pH, and highest preoperative lactate as independent predictors of mortality. (AUC = 0.896; 95% CI 0.834-0.958). A cutoff value of 0.436 demonstrated a specificity of 96%, sensitivity 59%, negative predictive value 97%, and overall accuracy of 93%.
Conclusion(s): The predictive model demonstrated excellent discrimination for NEC-attributable mortality in preterm infants. Gestational age, sex, inotrope requirement, lowest preoperative pH, and highest preoperative lactate were independent predictors, enabling early identification of high-risk infants and supporting timely clinical intervention.

 photo")