690 - Early Prediction of Surgical Need in Preterm Necrotising Enterocolitis: Toward Data-Driven Decision Support
Friday, April 24, 2026
5:30pm - 8:00pm ET
Publication Number: 1667.690
Dwayne Mascarenhas, The Hospital for Sick Children, Toronto, ON, Canada; Doaa Al-Dweik, The University of Western Ontario - Schulich School of Medicine & Dentistry, London, ON, Canada; Ujjwala Mantha, University of Toronto Temerty Faculty of Medicine, Toronto, ON, Canada; Shravan Kanaparthi, The Hospital for Sick Children, Toronto, ON, Canada; Bonny Jasani, The Hospital for Sick Children, Toronto, ON, Canada
Staff Physician & Assistant Professor Mount Sinai Hospital, Toronto Toronto, Ontario, Canada
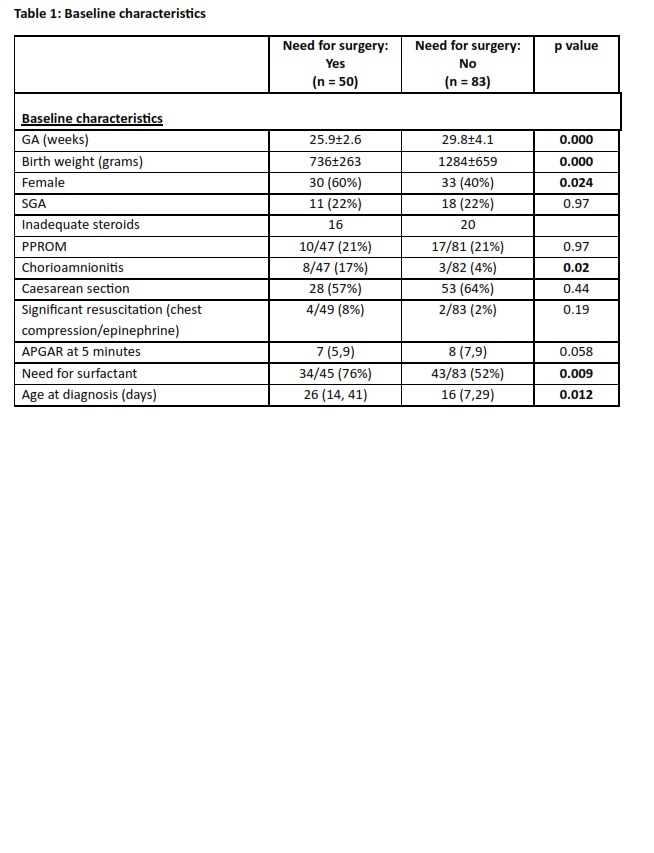
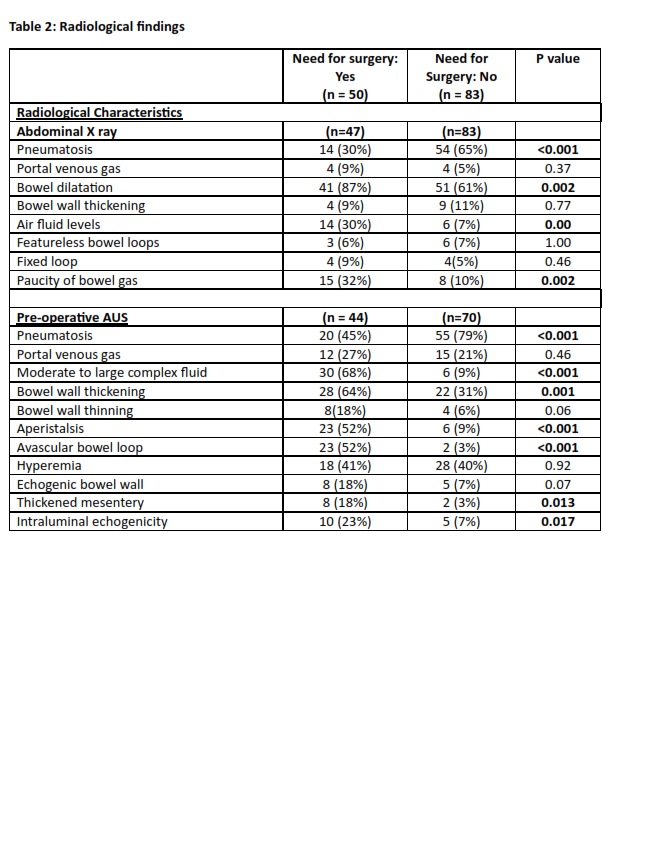
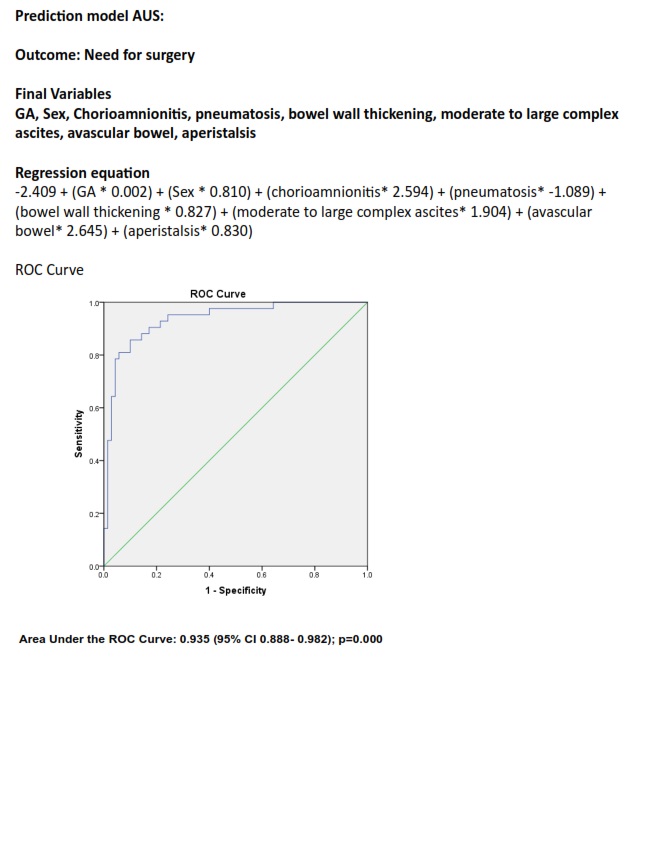
Background: Necrotizing enterocolitis (NEC) is a leading cause of mortality in preterm infants. A predictive model for need for surgery is needed to enable early risk stratification and guide timely interventions. Objective: To develop a predictive model based on clinical and ultrasound parameters for need for surgery in preterm infants with NEC. Design/Methods: This retrospective cohort study included preterm infants with NEC at a single quaternary neonatal intensive care unit between January 1, 2016 and June 30, 2024. Clinical and radiological variables prior to surgery were extracted to identify predictors of need for surgery. Multivariable logistic regression was used to develop the predictive model. The model performance was assessed using area under the receiver operating characteristic curve (AUC) and am optimal cutoff score was determined using Youden's index. Diagnostic accuracy metrics were calculated, and model co-efficients were used to construct a bedside risk prediction tool. Results: A total of 133 preterm infants with NEC were included (mean gestational age 28.4 ±4.1 weeks, birth weight 1078 ±605 grams), with 38% of the infants needing surgical intervention. Infants needing surgical intervention were significantly smaller, lighter, more likely to be female, and have exposure to chorioamnionitis. On ultrasound, the infants needing surgery were more likely to have bowel wall thickening, moderate to large complex ascites, avascular bowel, and aperistalsis. The final multivariable model identified gestational age, sex, chorioamnionitis, pneumatosis, bowel wall thickening, moderate to large complex ascites, avascular bowel, and aperistalsis as independent predictors of mortality. (AUC = 0.935; 95% CI 0.888- 0.982). A cutoff value of 0.507 demonstrated a specificity of 90%, sensitivity 64%, negative predictive value 97%, and overall accuracy of 88%.
Conclusion(s): The predictive model demonstrated excellent discrimination for need for surgery in preterm infants. Gestational age, sex, chorioamnionitis, pneumatosis, bowel wall thickening, moderate to large complex ascites, avascular bowel, and aperistalsis were independent predictors, enabling early identification of high-risk infants and supporting timely clinical intervention.

 photo")