65 - Cognitive Outcomes of Neonates with Hypoxic-Ischemic Encephalopathy Treated with Hypothermia: The Role of Socioeconomic Vulnerability
Friday, April 24, 2026
5:30pm - 8:00pm ET
Publication Number: 1058.65
Srishti Jayakumar, Children's Hospital of Philadelphia, Baltimore, MD, United States; Kathryn A.. Carson, Johns Hopkins University School of Medicine, Baltimore, MD, United States; Corina Mills, Johns Hopkins Bloomberg School of Public Health, Baltimore, MD, United States; Carolei Bryan, Johns Hopkins, Baltimore, MD, United States; Jordan R. Kuiper, George Washington University Milken Institute School of Public Health, Washington, DC, United States; Amii M.. Kress, Johns Hopkins Bloomberg School of Public Health, Baltimore, MD, United States; Gwendolyn Gerner, Kennedy Krieger Institute, Baltimore, MD, United States; Frances Northington, Johns Hopkins University School of Medicine, Baltimore, MD, United States; Amaris Keiser, Yale School of Medicine, Westport, CT, United States; Raul Chavez-Valdez, Johns Hopkins University School of Medicine, Baltimore, MD, United States; Vera Joanna Burton, Kennedy Krieger Institute, Baltimore, MD, United States
Attending Neonatologist Children's Hospital of Philadelphia Baltimore, Maryland, United States
Background: The role of maternal and neonatal factors in neurodevelopmental outcomes of infants surviving hypoxic-ischemic encephalopathy (HIE) treated with therapeutic hypothermia (TH) is established. However, there is limited literature examining how sociodemographic factors affect neurodevelopmental outcomes in these neonates. Objective: Our aim was to elucidate the relationship between county-level socioeconomic vulnerability and cognitive outcomes of neonates surviving HIE. Design/Methods: 43 infants with moderate to severe HIE who underwent TH were enrolled between 2010 and 2015. Using electronic medical records, we obtained clinical and sociodemographic characteristics including birth anthropometrics, gestational age, sex, cord pH, base deficit, Apgar scores at 1 and 5 minutes, brain MRI NICHD scores, peak creatinine and alanine transaminase levels in the first 24 hours. We used the CDC Social Vulnerability Index (SVI), a well-validated metric comprising four themes based on 16 US Census indicators to assess vulnerability for the infant's county of residence. We used Mullen scores comprising four subscales to assess cognitive outcomes at 24 months. Regression analyses were performed to assess the association of Mullen subscales with SVI adjusted for medical and individual sociodemographic factors found to be significant in univariate analysis, namely MRI NICHD scores, sex, and delivery mode. . Variables that were significant but collinear with MRI NICHD scores - Apgar scores and insurance status, were not included in the multivariate analysis. Results: Among infants with HIE treated with TH, we observed a significant negative adjusted association for CDC SVI scores and Mullen standard scores (p=0.04), specifically the Cognitive (p=0.04) and Visual Reception subscales (p=0.04). Of the components measured by the CDC SVI, Household Characteristics had the most significant negative adjusted association with Mullen standard scores (p= 0.04), Cognitive (p=0.04) and Visual Reception score (p=0.01) at 24 months. Within each theme and across all components of the Mullen, infants from areas with higher SVI had lower Mullen scores than infants from areas with less disadvantage.
Conclusion(s): County-level social vulnerability has a detrimental impact on neurodevelopmental outcomes of children with a history of neonatal HIE. Further research elucidating the specific contributions of these individual components will allow for identification of populations most at risk. This will aid the development of evidence-based, targeted interventions to improve outcomes and the realization of each child's full potential.

 photo")
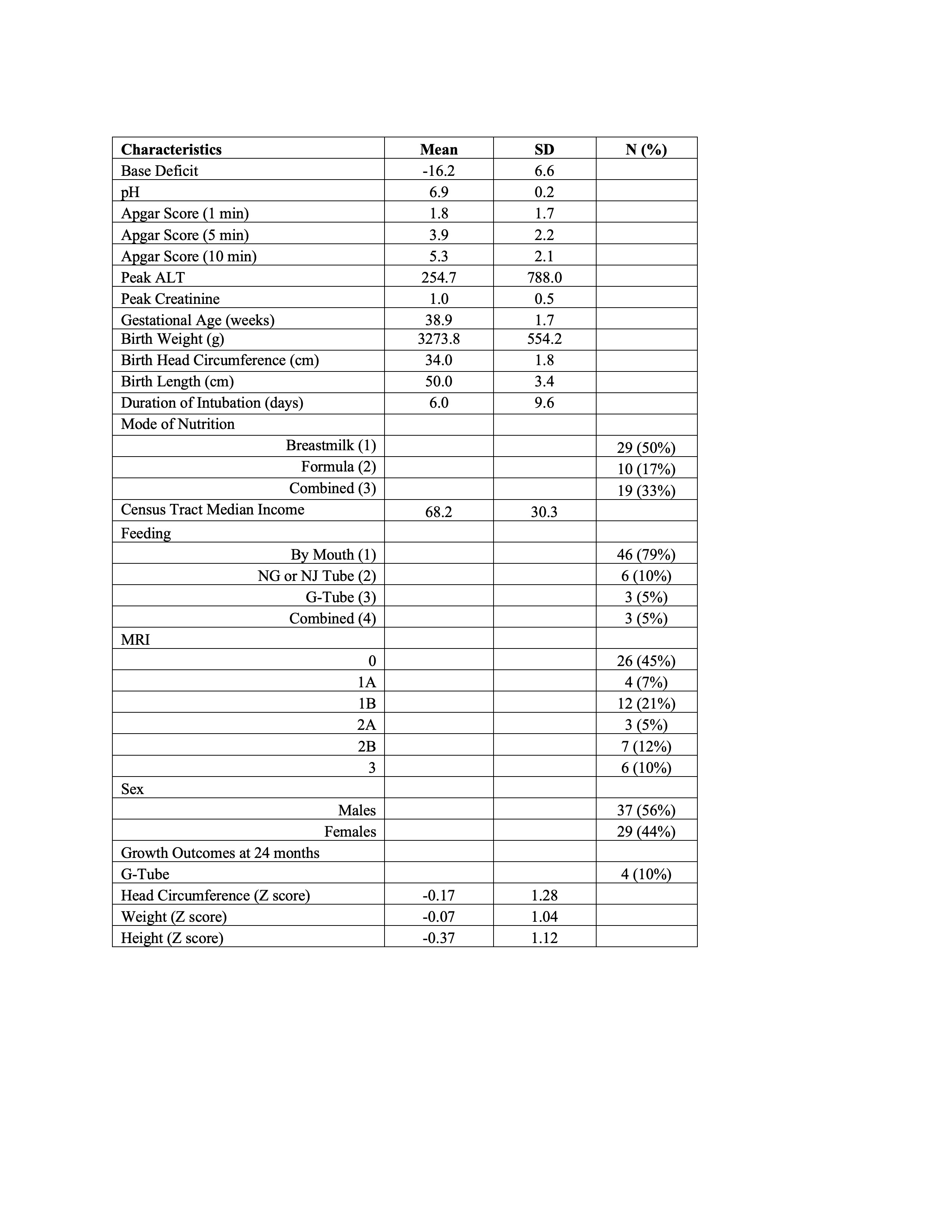 Participant Characteristics
Participant Characteristics