Session: Hospital Medicine Trainee Ongoing Projects: Clinical
TOP 44 - Transfer Call Characteristics of Pediatric Interfacility Transfers for Asthma
Saturday, April 25, 2026
3:30pm - 5:45pm ET
Publication Number: 2796.TOP 44
Revati Narawane, University of Texas at Austin Dell Medical School, Austin, TX, United States; Natalie Weston, Dell Children's Medical Center of Central Texas, AUstin, TX, United States; Sarah Walter, University of Texas at Austin Dell Medical School, Austin, TX, United States; Sanyukta Desai, University of Texas at Austin Dell Medical School, Austin, TX, United States
Fellow University of Texas at Austin Dell Medical School Austin, Texas, United States
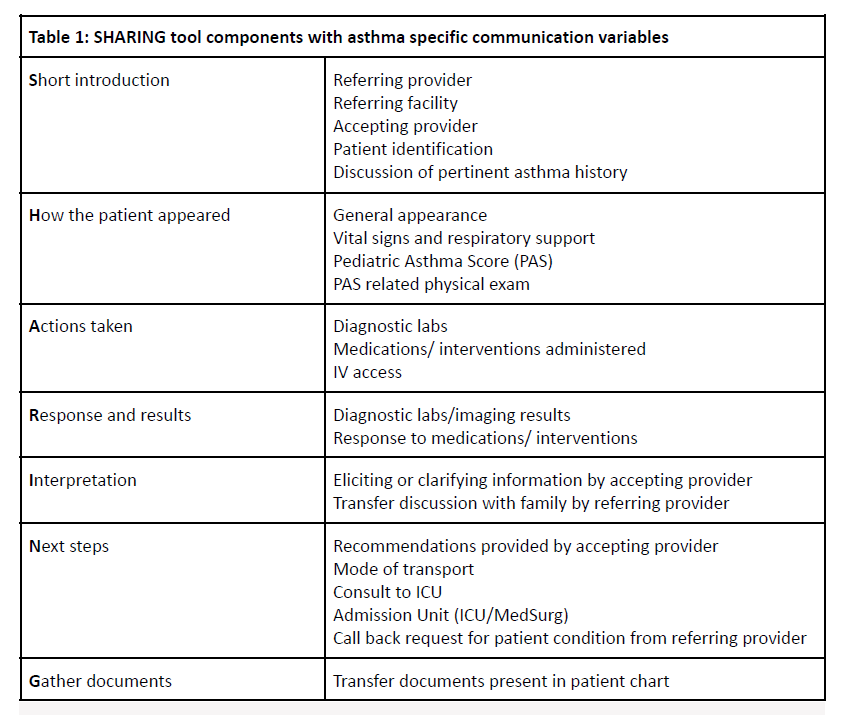
Background: Definitive care for common pediatric illnesses like asthma has shifted from community hospitals to tertiary care centers resulting in increased interfacility transfers. A quality handoff is essential in the safe transfer of patients between facilities. The "SHARING" tool, a standardized handoff intervention, has perceived benefits of reducing information deficits and appropriately triaging transfers (Table 1). There is, however, a gap in understanding of the utility of this tool in current practice. Objective: To describe the components of the SHARING handoff that were effectively communicated during pediatric interfacility asthma transfers. Design/Methods: This is a cross sectional study that includes pediatric patients transferred to a single tertiary care center with a primary diagnosis of asthma between February 1st, 2024 - February 28, 2025. We included children aged 3-18 years old who had an ED to inpatient (ICU/Med/Surg) interfacility transfer, while excluding ED to ED transfers and direct admissions from outpatient clinics. Patients who meet inclusion criteria were identified using the discharge diagnoses assigned on the transfer center dashboard as listed in Table 2. The patient and call details were then reviewed by two physicians to assess inclusion by confirming that the transfer was initiated for treatment of an asthma exacerbation. All identified call recordings were then listened to by two independent physicians.
We will describe the proportion of patients who received communication for each of the SHARING handoff tool components, as well as asthma-specific handoff communication using variables listed in Table 1. Additional variables include average call time, number of transfers to the ICU v. Med/Surg floors, ages of transferred patients. We anticipate that this will serve as a pilot study to guide future standardization and quality improvement of handoff in interfacility transfers of pediatric patients.
Table 1: SHARING tool components with asthma specific communication variables
Table 2: Primary Diagnoses as Assigned on Transfer Dashboard

.png)
