524 - Optimizing Antibiotic Therapy Duration in the Pediatric Emergency Department
Saturday, April 25, 2026
3:30pm - 5:45pm ET
Publication Number: 2509.524
Alexandra Debure, University of Miami Leonard M. Miller School of Medicine, Miami, FL, United States; Sarah Abushamma, University of Miami Leonard M. Miller School of Medicine, Miami, FL, United States; Kailynn DeRonde, Holtz Children's Hospital Jackson Memorial Hospital, Miami, FL, United States; Nicole A. McElroy, Holtz Children's Hospital Jackson Memorial Hospital, Miami, FL, United States; Brittany Jankauskas, Johns Hopkins All Children's Hospital, Largo, FL, United States; Maura Alvarez Baumgartner, University of Miami Leonard M. Miller School of Medicine, Miami, FL, United States; Brent D.. Rogers, Holtz Children's Hospital Jackson Memorial Hospital, Coral Gables, FL, United States
Medical Student University of Miami Leonard M. Miller School of Medicine Miami, Florida, United States
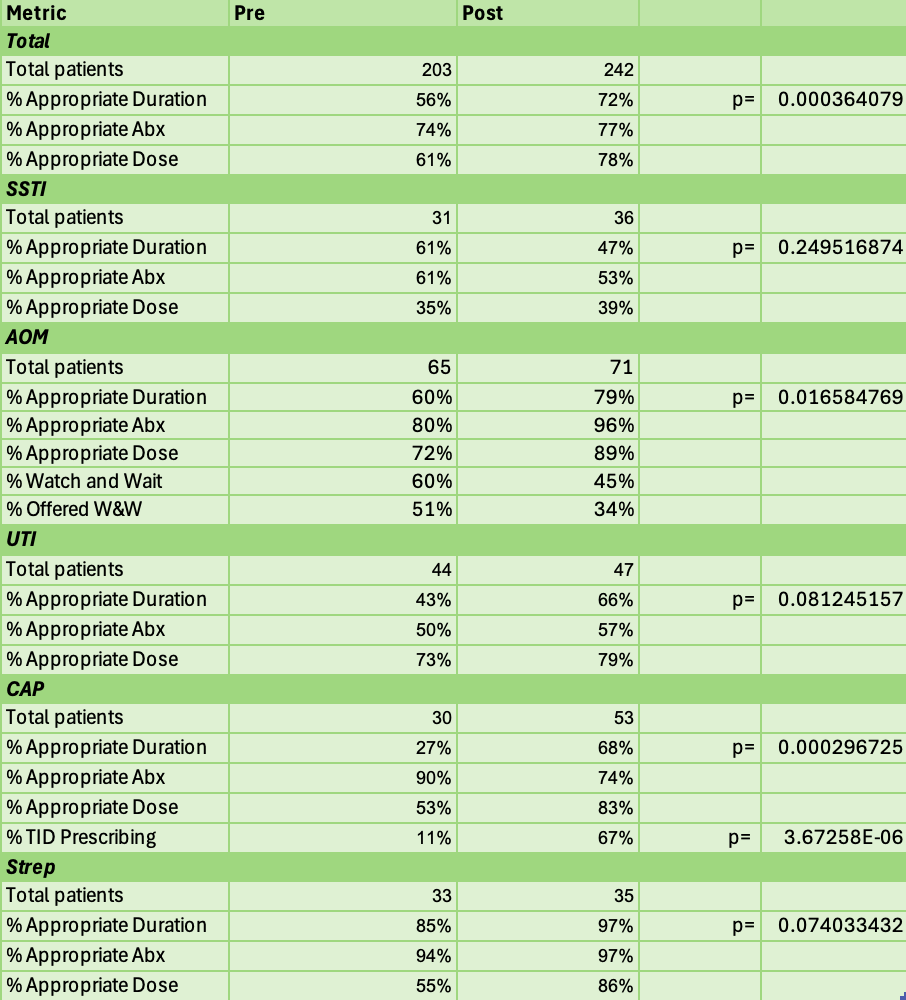
Background: More than 35,000 deaths are attributed to antibiotic-resistant infections in the United States each year. The pediatric emergency department (PED) accounts for approximately 30 million visits and seven million antibiotic prescriptions annually. Historically, most pediatric bacterial infections have been treated with antibiotic courses lasting 10 to 14 days. Prolonged antibiotic courses increase the risks of drug resistance and gastrointestinal complications. Recent studies suggest shorter durations are equally effective for community-acquired pneumonia (CAP), uncomplicated urinary tract infections (UTIs), skin and soft-tissue infections (SSTIs), and acute otitis media (AOM). A 'watch and wait' approach is safe for select cases of mild AOM. Objective: This QI initiative sought to improve prescriber adherence to evidence-based shorter durations of antibiotic therapy in the PED of an urban, academic teaching hospital through the introduction of easily accessible clinical guidelines. Design/Methods: A PDSA cycle was initiated in April 2024 to create an evidence-based chart outlining recommended dose, duration, and antibiotic choice by age, weight, and infection severity. This chart was designed by a multidisciplinary team and distributed to all attending and rotating resident physicians in monthly emails, a binder in the PED, QR codes, and on a centralized online hub. Charts of patients discharged with AOM, CAP, UTI, group A streptococcal pharyngitis (GAS), or SSTI from September to November 2024 (preintroduction) and September to November 2025 (postintroduction) were reviewed. The primary outcome was adherence to recommended antibiotic duration; secondary outcomes included antibiotic choice, proper dosing, and adherence to "watch and wait" when applicable. Results: A total of 203 pre- and 242 post-intervention PED charts were reviewed. Overall adherence to recommended antibiotic duration improved from 56% to 72% (p < 0.01), driven by gains in AOM (60→79%, p< 0.05) and CAP (27→68%, p< 0.01). Non-significant increases occurred for UTI (43→66%) and GAS (85→97%), while SSTI adherence declined (61→47%). In CAP, evidence-based TID dosing for our community's S. pneumoniae isolates rose significantly (11→67%, p< 0.01).
Conclusion(s): A low-cost tool improved adherence to antibiotic duration and prescribing consistency in the PED, especially for AOM and CAP. Providing easily accessible, evidence-based resources to educate providers on current guidelines offers a feasible approach to improving antibiotic stewardship, though alternate strategies may be needed for infections with variable management, such as SSTIs.
Table 1. Descriptive data for pre- and post-intervention.
Table 2. Complete prescribing information circulated to pediatric emergency department prescribers. Antibiotics Complete.pdfThis table was named the "complete version" as it contained details regarding pediatric dosing for antibiotics. Both this table and the following table were available in every modality in which the resource was provided.
Table 3. Simplified prescribing information circulated to pediatric emergency department prescribers. Antibiotics Simplified.pdfThis table was named the "simplified version" as it contained only the duration of time for the antibiotic to be prescribed and the name of the antibiotic, without any dosing information. Both this table and the previous table were available in every modality in which the resource was provided.