566 - Outcomes Of Procedural Sedation In Infants Outside The Operating Room
Saturday, April 25, 2026
3:30pm - 5:45pm ET
Publication Number: 2551.566
NIrupama Kannikeswaran, Central Michigan University, Children's Hospital of Michigan, Detroit, MI, United States; Rebecca K. Burger, Emory University School of Medicine, Atlanta, GA, United States; Mark Roback, University of Colorado School of Medicine, Denver, CO, United States; Ewa Sucha, CHEO, Ottawa, ON, Canada; Nick Barrowman, Children’s Hospital of Eastern Ontario Research Institute, Ottawa, ON, Canada; Maala Bhatt, Children's Hospital of Eastern Ontario, Ottawa, ON, Canada
Professor of pediatrics and emergency medicine Central Michigan University, Children's Hospital of Michigan Northville, Michigan, United States
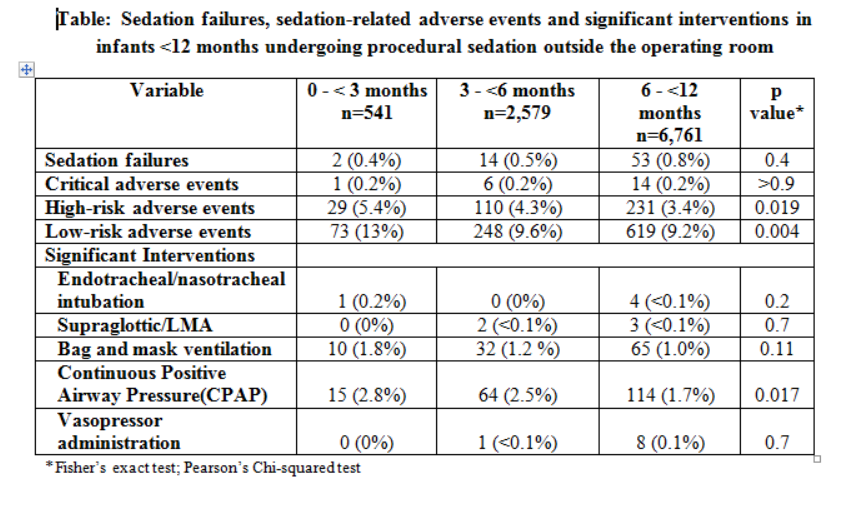
Background: Infants comprise approximately 10% of all children who undergo procedural sedation outside the operating room. Infants often require higher doses of sedatives and are at increased risk of sedation-related adverse events (AEs) and sedation failures compared to older children. Prior studies evaluating sedation efficacy and outcomes in infants are limited by small sample sizes and single-center enrollment. Objective: To describe and compare sedation safety and failures in infants under 12 months who underwent procedural sedation outside the operating room. Design/Methods: We conducted a multicenter cohort study of infants who underwent procedural sedation outside the operating room between 04/27/2020 - 12/31/2024, using the prospectively collected Pediatric Sedation Research Consortium database. The primary exposure was infant age group (0- < 3months, >3-6 months, 6-12 months). The primary outcome was the incidence of any sedation-related AEs, serious AEs (critical and high-risk), significant interventions performed in response to AEs, and sedation failures. Results: A total of 9,881 infants were analyzed (0- < 3 months: 541; 3- < 6 months: 2,471; 6-12 months: 6,761). Median weight was 8.0 kg (IQR 6.8-9.05), and 56% were male. Comorbid medical conditions were present in 69% of infants and 5.2% had a history of prematurity. The most common indications for sedation were imaging (83%), hematologic procedures (5.2%) and neurologic procedures (4.6%). High-risk (5.4% vs. 4.3% vs. 3.4%; p=0.019) and low-risk AEs were more frequent (13% vs. 9.5% vs.9.6%; p=0.004) in infants aged 0- < 3 months compared to the other two age groups. The frequency of critical AEs was rare and did not differ significantly by age group (0.2% vs. 0.2% vs. 0.2%; p>0.9). Sedation failures were uncommon (0.4% vs. 0.5% vs. 0.8%; p=0.4). Though significant interventions were rare, need for continuous positive airway pressure was slightly more common in infants 0- < 3 months (2.8% vs.2.5% vs. 1.7%; p=0.017) (Table).
Conclusion(s): Although sedation-related low-risk AEs were common, critical and high-risk AEs, were rare. Sedation failures and need for significant interventions were uncommon across the age groups. These findings highlight the overall safety of procedural sedation in infants outside the operating room when performed within dedicated pediatric sedation systems and in the hands of experienced providers.
Table: Sedation failures, sedation-related adverse events and significant interventions in infants <12 months undergoing procedural sedation outside the operating room