612 - Implementing enteral hydration and nutrition via nasogastric tube in children hospitalized with bronchiolitis
Saturday, April 25, 2026
3:30pm - 5:45pm ET
Publication Number: 2597.612
Alyssa Coffin, Boston Children's Hospital, Boston, MA, United States; Patricia Stoeck, Boston Children's Hospital/Harvard Medical School, Boston, MA, United States; Meghan C. Kostyk, Boston Children's Hospital, Boston, MA, United States; Daniel J. Kats, Boston Children's Hospital, Boston, MA, United States; Caroline Kohler, Boston Children's Hospital, Boston, MA, United States; Loren W. Aiello, Boston Children's Hospital, Boston, MA, United States; Elizabeth King, Boston Children's Hospital, Boston, MA, United States; Amanda Lossner, Boston Children's Hospital, Boston, MA, United States; Amanda Growdon, Boston Children's Hospital, Boston, MA, United States; Niloufar Paydar-Darian, Boston Children's Hospital, Boston, MA, United States; Maria Biancarelli, Boston Children's Hospital, SOUTH WALPOLE, MA, United States; Jason Levy, Boston Children's Hospital, Needham, MA, United States; Joel H. Hudgins, Brown Emergency Medicine, Milton, MA, United States; Lisa Rickey, Boston Children's Hospital, Boston, MA, United States
Instructor of Pediatrics Harvard Medical School, Boston Children's Hospital Boston, Massachusetts, United States
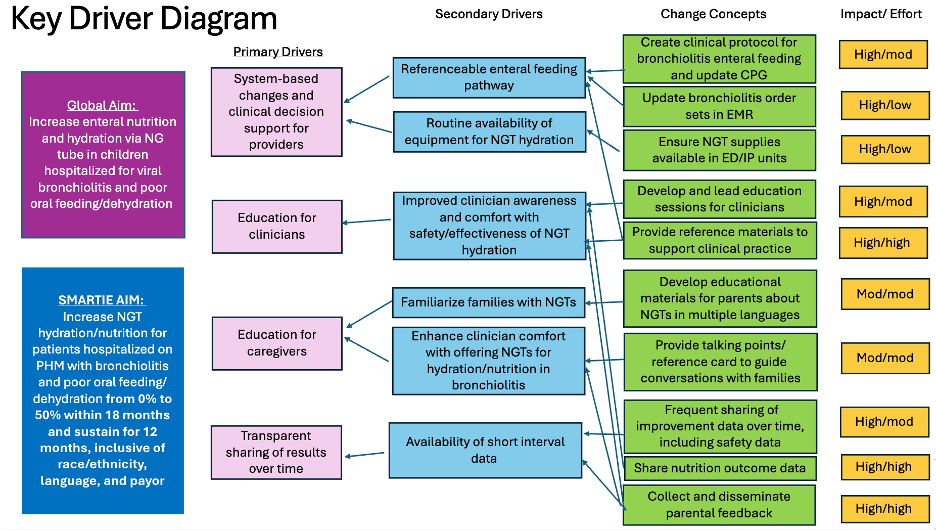
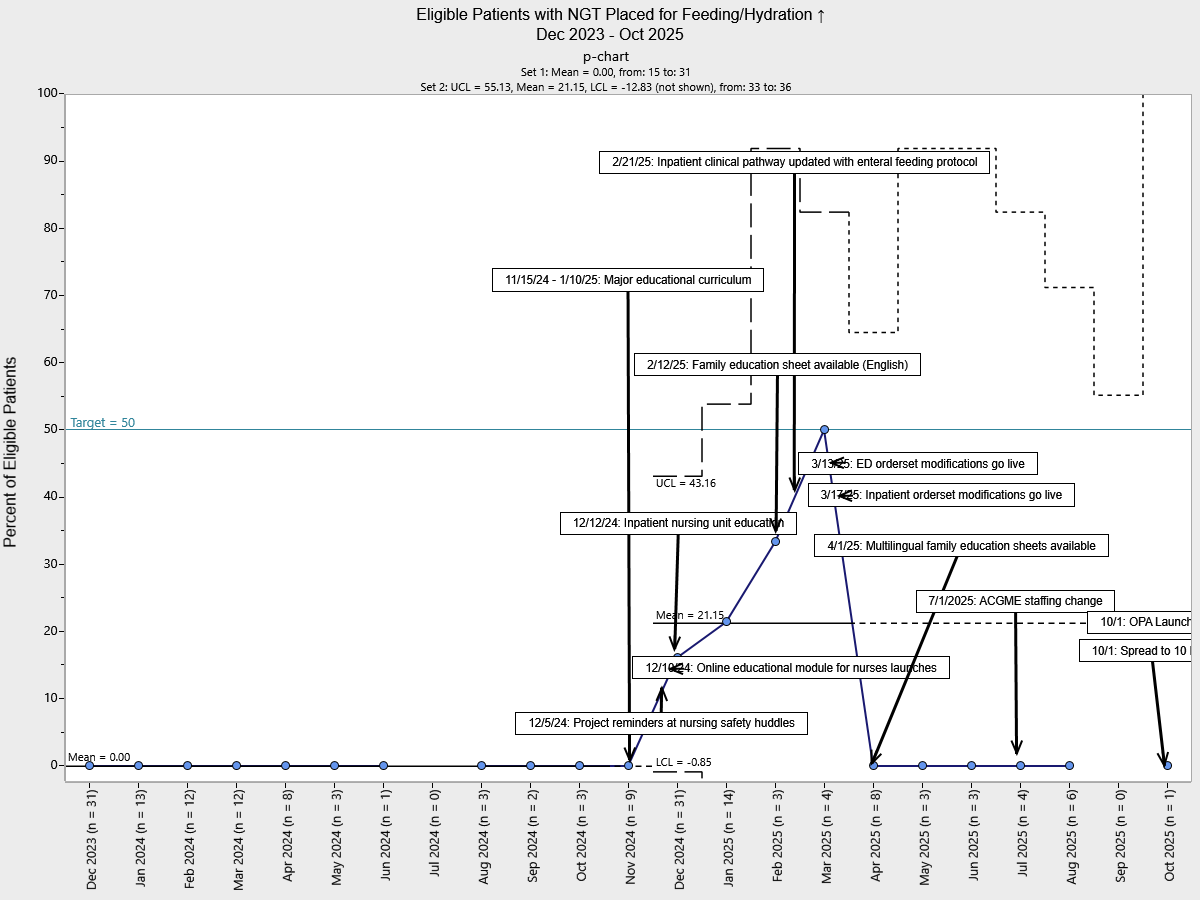
Background: Enteral feeding and hydration via nasogastric tube (NGT) is a safe, effective, and well-tolerated alternative to intravenous (IV) hydration in children hospitalized with bronchiolitis. However, current practice in our institution utilizes exclusively IV fluids to support hydration in children with bronchiolitis who have inadequate oral intake. Objective: Our SMARTIE aim is to implement NGT hydration/nutrition for children hospitalized with bronchiolitis and inadequate oral intake on Pediatric Hospital Medicine teams from 0% to a 50% within 18 months, inclusive of race/ethnicity, language, and payor. Design/Methods: Utilizing the Model for Improvement, a multidisciplinary key partner team developed bundled interventions to facilitate this practice change. A key driver diagram guided the development of interventions including integration of an enteral feeding protocol into a local Clinical Pathway, updates to order sets in the electronic medical record, creation of clinical decision support tools, multimodal education for providers and nurses, and multilingual parent/caregiver educational references (Figure 1). We utilized Plan-Do-Study-Act cycles to implement and study the effect of our interventions. Our primary outcome measure was the percentage of eligible patients who receive NGTs for feeding/hydration, tracked over time using a statistical process control p-chart. Our process measure was the completion rate of an online educational module for nurses. Our balancing measures included length of stay (LOS) and unplanned intensive care unit (ICU) transfers. Results: Over the first 11 months of the intervention period, NGT utilization in children with bronchiolitis increased from a baseline of 0% to a mean of 21%, meeting criteria for special cause variation following the interventions (Figure 2). We achieved a 95.5% completion rate for the nursing educational module (process measure). There were no significant changes in LOS or ICU transfers (balancing measures) that could not be attributed to seasonal variation. There were no differences in intervention rates by language or insurance payor. Due to small sample size, we were unable to assess meaningful differences by race/ethnicity.
Conclusion(s): This improvement work was rapidly implemented in response to national IV fluid shortages. Consequently, early improvements have been achieved largely through educational efforts alone. In preparation for the upcoming bronchiolitis season we have designed and implemented systems-based changes that we anticipate will support more robust and sustainable improvement toward our goal.
Figure 1: Key Driver Diagram for increasing use of nasogastric tubes for hydration and nutrition in children hospitalized with bronchiolitis.
Figure 2: Statistical process control p-chart showing eligible patients with bronchiolitis receiving nasogastric hydration on Pediatric Hospital Medicine teams

 Credit")
 photo")