115 - Association of Caffeine Citrate Administration with Necrotizing Enterocolitis in Infants < 32 Weeks' Gestation: A Retrospective Cohort Study
Saturday, April 25, 2026
3:30pm - 5:45pm ET
Publication Number: 2110.115
Xiaoshan Hu, Nanjing Women and Children's Healthcare Hospital, Nanjing, Jiangsu, China (People's Republic); Qifeng Wang, Women’s Hospital of Nanjing Medical University, Nanjing, Jiangsu, China (People's Republic); Li Zhu, CHildren's hospital of Fudan university, Shanghai, Shanghai, China (People's Republic); Dan Dang, Dan Dang, Changchun, Jilin, China (People's Republic); Jie yang, Fudan Children's Hospital, Shanghai, Shanghai, China (People's Republic)
Pediatric attending physician Nanjing Women and Children's Healthcare Hospital Nanjing, Jiangsu, China (People's Republic)
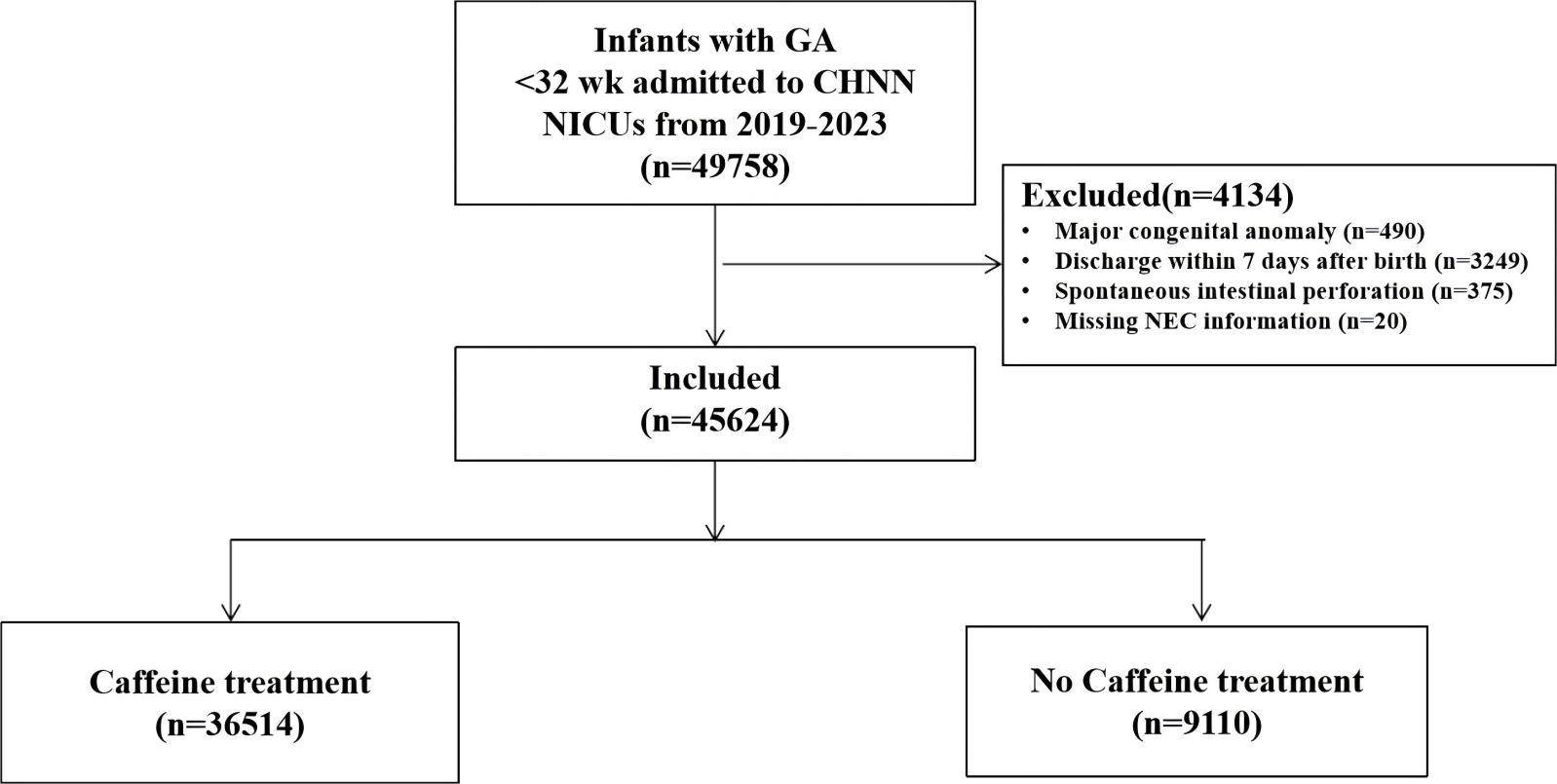
Background: Caffeine is accepted to be a treatment for apnea of prematurity (AOP). However, its effect on necrotizing enterocolitis (NEC) is still controversial at present. To examine the association between caffeine citrate administration and NEC in very preterm infants (VPIs). Objective: To examine the association between caffeine citrate administration and necrotizing enterocolitis(NEC) in very preterm infants(VPIs). Design/Methods: This multicenter retrospective cohort study was conducted from January 1, 2019, to December 31, 2023, at level III neonatal intensive care units (NICU) participating in the Chinese Neonatal Network (CHNN). Participants included neonates born with a gestational age (GA) less than 32 weeks. Participants were divided into two groups: the non-caffeine group and the caffeine group, based on their exposure to caffeine citrate after birth. The primary outcomes were the incidence of NEC (≥stage IIA) and surgical NEC during the hospitalization in the NICU. The secondary outcomes were severe neonatal morbidities, including severe intraventricular hemorrhages, severe retinopathy of prematurity, late-onset sepsis, bronchopulmonary dysplasia, and death, and other variables, including days of parenteral nutrition and NICU stay. Results: Compared with VPIs who did not receive caffeine citrate, those who did have lower GA and birth weight, a higher rate of inborn, small for gestational age, antenatal corticosteroid, 1-minute Apgar score ˂ 8, higher TRIPIS score, blood transfusion, and vasopressors usage. Caffeine citrate exposure did not affect the incidence of NEC (≥ stage IIA) between groups; however, its early administration (within 72 hours after birth) was associated with a lower incidence of surgical NEC (adjusted odds ratio [aOR], 0.76; 95% CI, 0.64-0.89). In subgroup analysis, caffeine citrate administration was associated with a reduction incidence of NEC (≥ stage IIA) among VPIs receiving invasive ventilation at admission (aOR, 0.73; 95% CI, 0.58-0.93) and vasopressors (aOR, 0.64; 95% CI, 0.52-0.78).
Conclusion(s): While the incidence of NEC (≥ stage IIA) in VPIs has not been affected, early caffeine citrate administration (within 72 hours after birth) was associated with a reduced incidence of surgical NEC. Furthermore, among VPIs who received invasive ventilation at admission and vasopressors, the administration of caffeine citrate was observed to potentially decrease the occurrence of NEC (≥ stage IIA).
Figure 1: Flow Chart
Figure 2. Subgroup analysis of caffeine treatment on NEC (≥ stage ⅡA)

.jpg)
