348 - Factors Contributing to Tracheostomy in Extremely Low Birthweight Infants with Moderate to Severe Bronchopulmonary Dysplasia - a Single-Center Study
Saturday, April 25, 2026
3:30pm - 5:45pm ET
Publication Number: 2337.348
Julianne M. Cottrell, Baylor College of Medicine, Houston, TX, United States; Monika S.. Patil, Baylor College of Medicine, Houston, TX, United States; Joseph Hagan, Baylor College of Medicine, Houston, TX, United States; Maya Brasher, Baylor College of Medicine, Houston, TX, United States
Pediatrics Resident Baylor College of Medicine Houston, Texas, United States
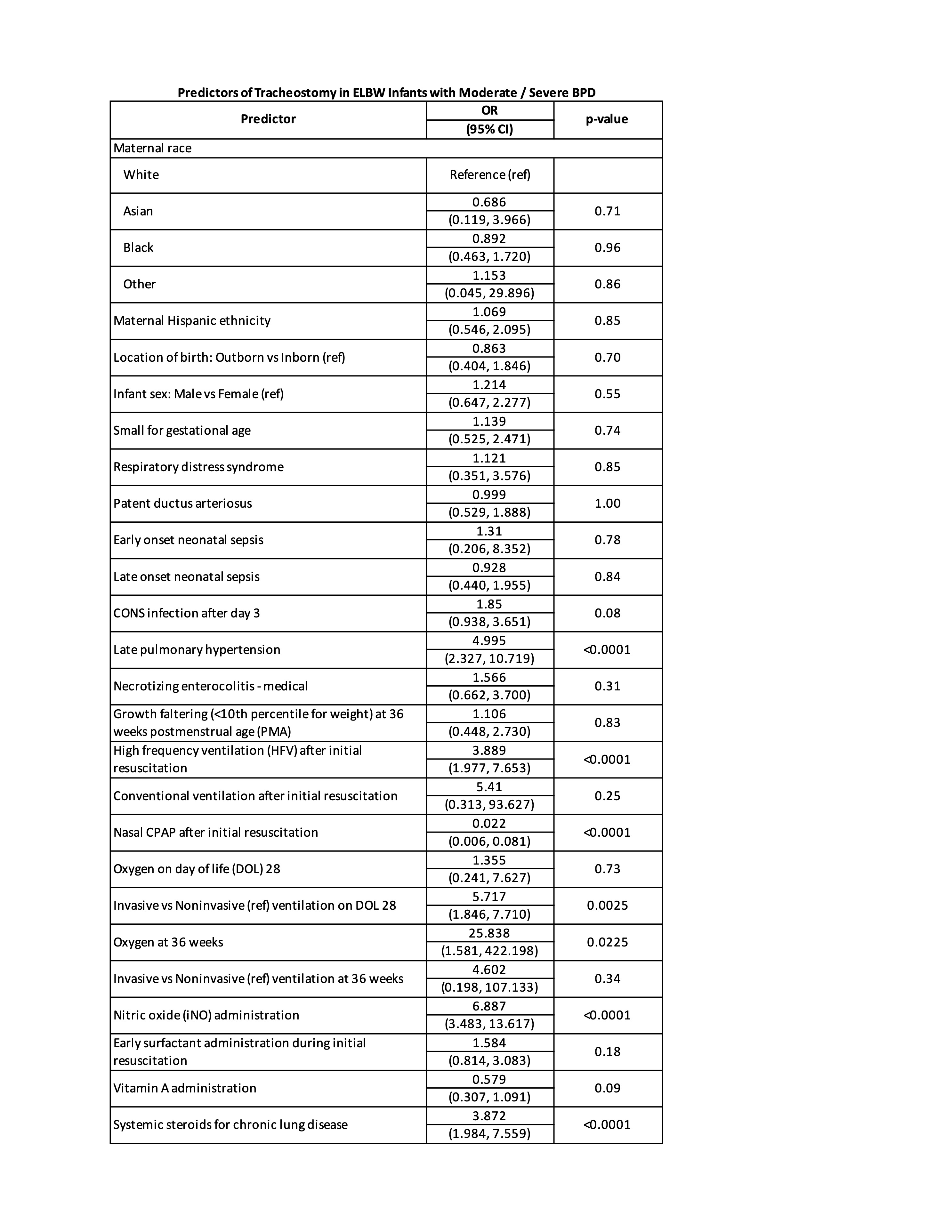
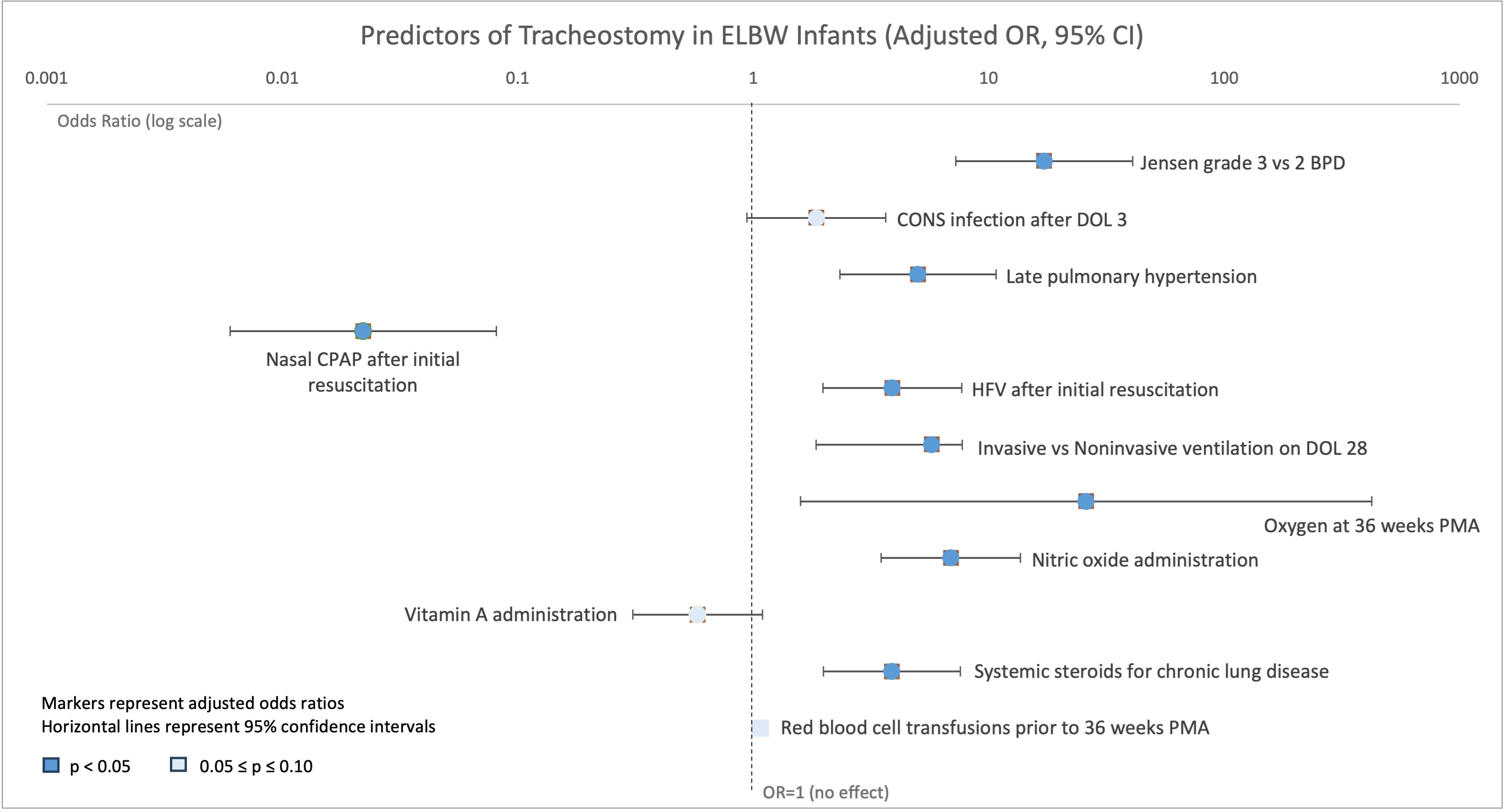
Background: Bronchopulmonary dysplasia (BPD) is the most common complication of prematurity. Extremely low birthweight (ELBW, < 1000g birthweight) infants face the highest risk of BPD with the possibility of long-term dependence on mechanical ventilation. With more ELBW infants surviving with BPD, understanding factors contributing to tracheostomy is essential to improve clinical management, patient outcomes, and accurate prognostication. Objective: We aimed to determine factors associated with tracheostomy in ELBW infants with moderate to severe BPD. Design/Methods: In this single-center, retrospective, descriptive study, we analyzed data from ELBW infants with moderate to severe (Jensen grade 2 or 3) BPD at a quaternary referral hospital from 1/1/2013 to 12/31/2023. Infants who died prior to discharge or had major congenital anomalies were excluded. Data were extracted from Vermont Oxford Network and Children's Hospitals Neonatal Consortium databases, and from electronic chart review after obtaining institutional review board approval. Logistic regression analysis examined the association of predictors with tracheostomy due to the relatively low proportion of infants requiring tracheostomy, and multivariable models were fit to examine the association of each predictor with tracheostomy after controlling for birthweight (BW). Results: Of 510 ELBW infants, 43 (8.4%) required tracheostomy. Factors independently associated with tracheostomy included late pulmonary hypertension (>36 weeks post menstrual age [PMA]), high-frequency ventilation after resuscitation, systemic steroids for chronic lung disease, nitric oxide therapy, and oxygen at 36 weeks PMA (Table 1). Jensen grade 3 versus grade 2 BPD was associated with higher odds of requiring tracheostomy (Table 1). Infants requiring tracheostomy had longer duration of assisted ventilation (94 versus 42 days, p< 0.0001), were older at discharge (median of 270 versus 141 days of life, p< 0.0001), and were more likely to need a gastric tube (Table 1). Nasal CPAP use after initial resuscitation was significantly protective (Figure 1).
Conclusion(s): We found tracheostomy was most strongly linked to late pulmonary hypertension, prolonged invasive ventilation, oxygen requirement at 36 weeks PMA, and need for nitric oxide and systemic steroids, while nasal CPAP use after initial resuscitation was protective. Findings suggest that severity of respiratory disease predominantly contributes to risk for tracheostomy. Multi-center studies may help address patient volume and generalizability of findings, improving risk stratification and counseling for families of infants with BPD.
Table 1: Predictors of Tracheostomy in ELBW Infants with Moderate / Severe BPD
Figure 1: Predictors of Tracheostomy in ELBW Infants (Adjusted OR, 95% CI)

 photo")