547 - Identifying Practice Patterns in the Treatment of Frequently Relapsing and Steroid Dependent Childhood Nephrotic Syndrome
Monday, April 27, 2026
8:00am - 10:00am ET
Publication Number: 4535.547
Megan E. Woods, Oakwood University, Grand Ledge, MI, United States; Bradley P. Dixon, University of Colorado School of Medicine, Aurora, CO, United States; Caroline Gluck, Nemours Children's Health, Wilmington, DE, United States; Mark Mitsnefes, Cincinnati Children's Hospital Medical Center, Cincinnati, OH, United States; Carla M.. Nester, University of Iowa Stead Family Children's Hospital, Iowa City, IA, United States; Alicia Neu, The Johns Hopkins University School of Medicine, Baltimore, MD, United States; Daryl Okamura, Seattle Children's, Seattle, WA, United States; William E.. Smoyer, Nationwide Children's Hospital, Powell, OH, United States; Michael Somers, Boston Children's Hospital, Boston, MA, United States; Brian Stotter, Washington University in St. Louis School of Medicine, St. Louis, MO, United States; Priya S. Verghese, Northwestern University The Feinberg School of Medicine, Chicago, IL, United States; Michelle Denburg, Children's Hospital of Philadelphia, Philadelphia, PA, United States; Madhura Pradhan, Perelman School of Medicine at the University of Pennsylvania, Philadelphia, PA, United States
Undergraduate Student Oakwood University Grand Ledge, Michigan, United States
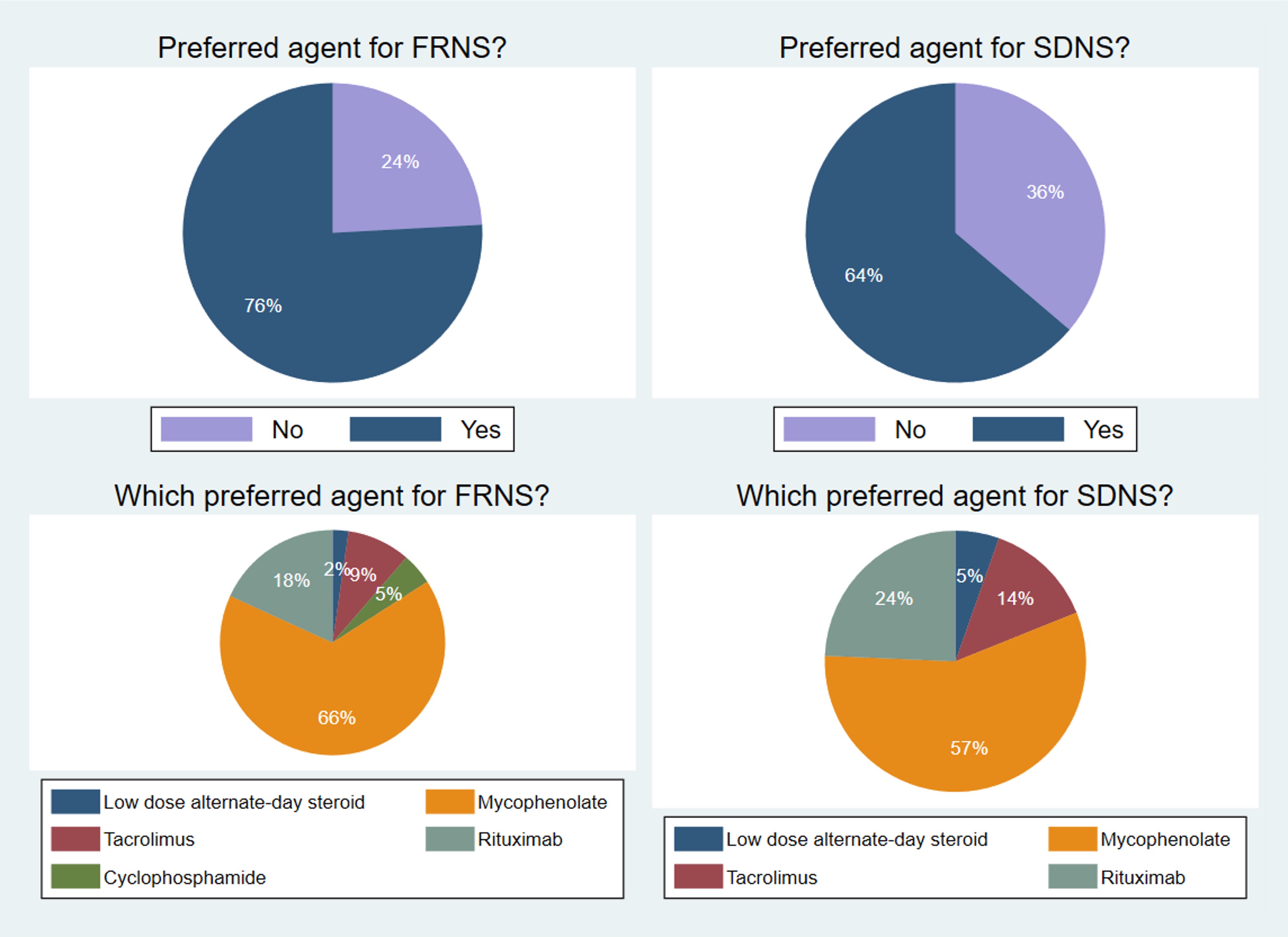
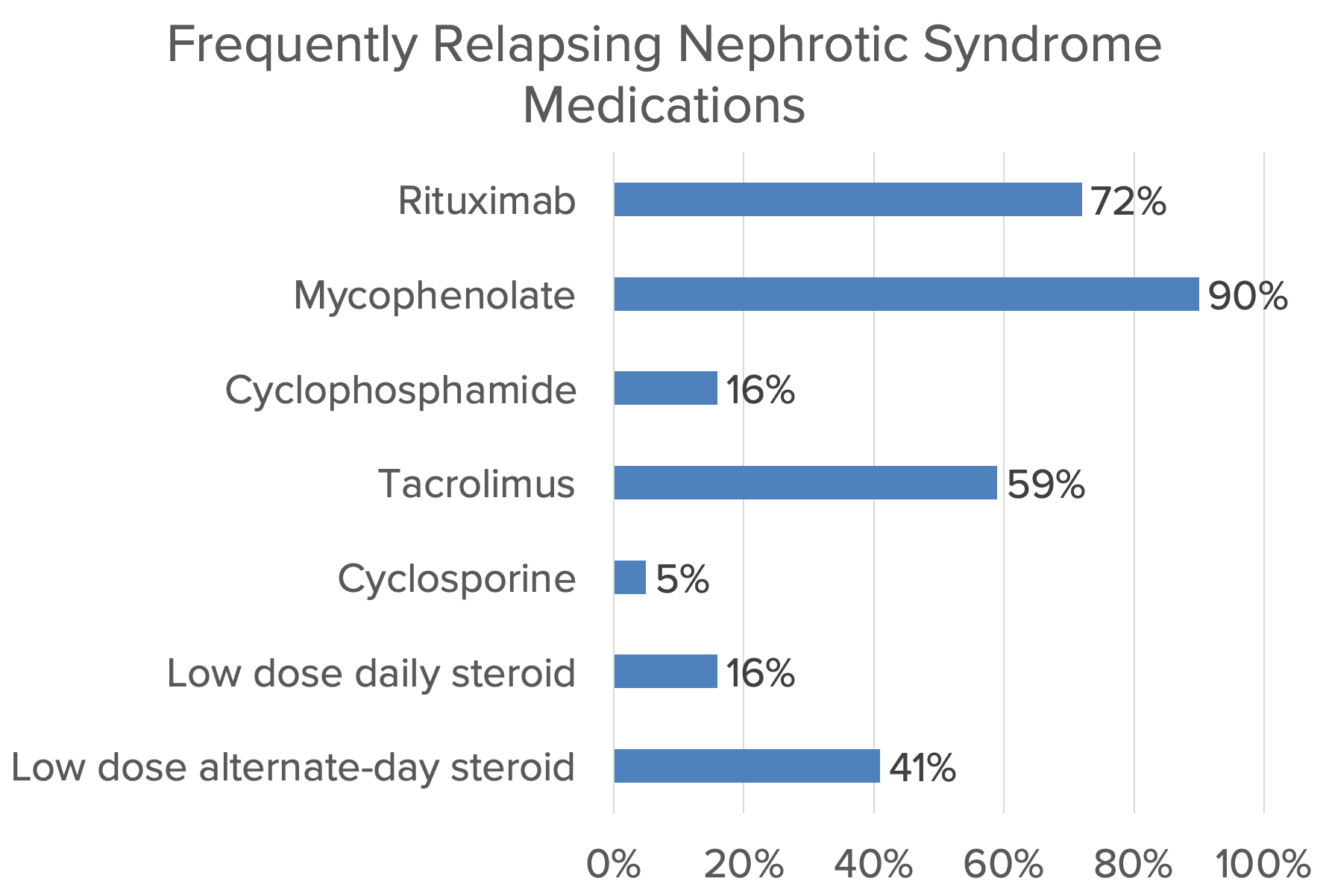
Background: Many children with nephrotic syndrome experience frequent relapses or steroid dependence. Treatment of frequently relapsing (FRNS) and steroid dependent nephrotic syndrome (SDNS) involves the use of steroid-sparing agents to mitigate adverse effects resulting from cumulative high dose steroid exposure. Recently published International Pediatric Nephrology Association (IPNA) guidelines recommend using cyclophosphamide, calcineurin inhibitors or mycophenolate mofetil, with rituximab as a second line agent if the first line agent fails to maintain remission, but the relative usage of these agents is not well described. Objective: To describe the current landscape of and variability in practice patterns in the treatment of FRNS/SDNS in the United States. Design/Methods: A REDCap survey was designed and administered to pediatric nephrologists and advanced practice providers in the Glomerular Learning Network (GLEAN) collaborative that includes 11 large US pediatric hospitals. 58 responses were analyzed using standard descriptive statistics. Results: Figure 1 shows the medications used by respondents to treat FRNS and SDNS. For FRNS, the most used agents were mycophenolate (90%) > rituximab (72%) > tacrolimus (59%). For SDNS, the most used agents were mycophenolate (79%) = rituximab (79%) > tacrolimus (62%). 76% of respondents reported a preferred agent to treat FRNS, while 64% had a preferred agent to treat SDNS (Figure 2). Of respondents with a preferred agent: 66% and 57% selected mycophenolate for treatment of FRNS and SDNS, respectively; 18% and 24% selected rituximab for FRNS and SDNS, respectively; and 9% and 14% selected tacrolimus for FRNS and SDNS, respectively. The most commonly reported factors influencing provider choice were adherence (91%) and age (52%). 90% of providers responded that family preference influenced their choice of medication.
Conclusion(s): There is moderate variability in provider preference and practice patterns for steroid-sparing immunosuppression in FRNS and SDNS. Choice of agent involves a shared decision-making process in which patient/family preference plays an important role.

 photo")
.png)