686 - Multidimensional predictors of early neurodevelopmental outcomes in infants with Chiari II malformation and myelomeningocele
Saturday, April 25, 2026
3:30pm - 5:45pm ET
Publication Number: 2669.686
Rutvi Vyas, Boston Children's Hospital, Boston, MA, United States; Matheus Dorigatti Soldatelli, Mass General Brigham, Boston, MA, United States; Henry A.. Feldman, Boston Children's Hospital, Boston, MA, United States; Benjamin C.. warf, Boston Children's Hospital, Harvard Medical School, Boston, MA, United States; Jennifer T. Queally, Boston Children's Hospital, Boston, MA, United States; P. Ellen grant, Boston Children's Hospital, Boston, MA, United States; Pei-Yi Lin, Boston Children's Hospital, Cambridge, MA, United States
Assistant Professor Boston Children's Hospital Harvard Medical School Cambridge, Massachusetts, United States
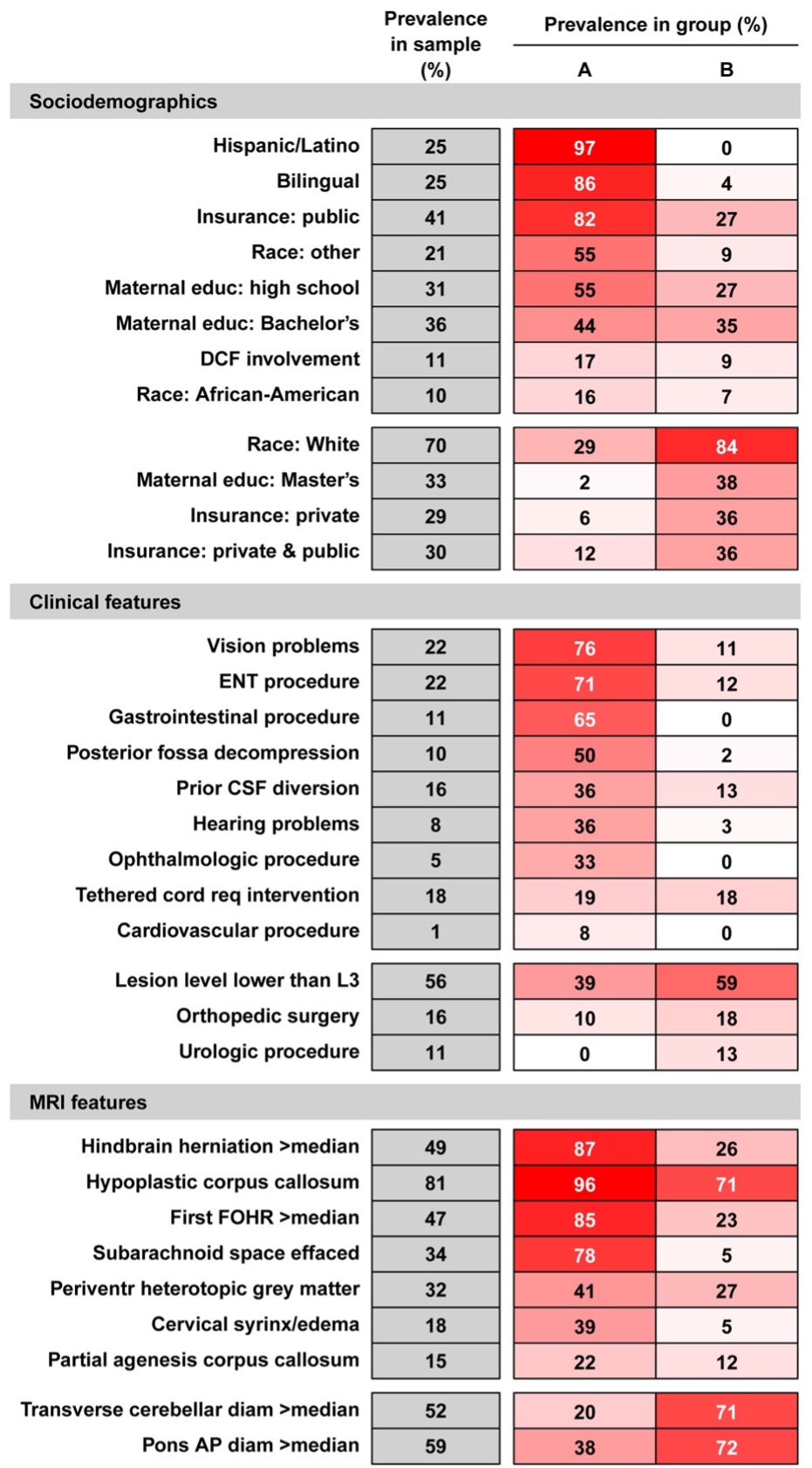
Background: Infants with Chiari II malformation (CM2) and myelomeningocele (MMC) face significant neurodevelopmental (ND) challenges, yet prognostic factors remain incompletely characterized in the era of endoscopic third ventriculostomy with choroid plexus cauterization (ETV/CPC) as standard-of-care hydrocephalus (HC) treatment. Objective: To evaluate how HC management, prenatal MMC repair, sociodemographic factors, clinical complexity and brain MRI features collectively influence early ND outcomes in CM2/MMC infants. Design/Methods: This is a retrospective cohort study of 73 infants with CM2 and MMC repair born July 2010-July 2021, followed at Boston Children's Hospital Spina Bifida Center. Sociodemographic and clinical data were extracted from medical records. MRI features were assessed by expert neuroradiological review (Table1). ND outcomes were assessed longitudinally using Bayley Scales of Infant and Toddler Development 3rd edition (BSID-3) (median,IQR:4,2-4 assessments/patient). Latent class analysis (LCA) reduced sociodemographic, clinical and MRI predictors into dichotomies (Figure1). Linear mixed-effects model examined multivariable associations of HC management (ETV/CPC, VPS or no intervention), prenatal repair of MMC and LCA-derived sociodemographic, clinical and MRI groups with BSID-3 scores, adjusting for age and sex (Table2). Results: Among 237 BSID-3 assessments (mean age: 17±8mo, range: 4-30mo), age at assessment inversely correlated with cognitive and motor scores (both p< 0.001). Females had higher motor scores (p=0.02). HC management predicted outcomes: VPS-dependent infants had lower cognitive scores than those without intervention (p=0.007) and lower motor scores than both no-intervention (p=0.004) and successful ETV/CPC groups (p=0.04). Each predictor domain contributed independently: sociodemographic group with greater environmental support predicted higher cognitive (p=0.008) and language scores (p=0.002); clinical group with lower lesion levels and fewer comorbidities predicted higher language (p=0.004) and motor scores (p=0.006); MRI group without evidence of HC and with larger cerebellar diameters predicted higher cognitive and motor scores (both p=0.04).
Conclusion(s): In CM2/MMC, HC management, sociodemographic support, clinical complexity, and MRI features each independently shape early ND trajectories. Notably, successful ETV/CPC outcomes were comparable to no intervention, while VPS dependence predicted worse outcomes. Findings support integrated, multidimensional risk stratification to optimize prognostication, guide early intervention timing, and target family and community supports.
Table 1: (A) Sociodemographic, (B) Clinical and (C) MRI characteristics of all patients
Figure 1: Latent Class Analysis (LCA) of Sociodemographic, Clinical and MRI features
Table 2: Multi-variate association of sociodemographic, surgical, clinical and MRI factors with ND outcome

 photo")
.png)
.png)
