659 - Cognitive Trajectories for Children Born Very Preterm to Age 8
Saturday, April 25, 2026
3:30pm - 5:45pm ET
Publication Number: 2642.659
Buse Bedir, BC Children's Hospital, Vancouver, BC, Canada; Ting Guo, The Hospital for Sick Children, Toronto, ON, Canada; Jessie van Dyk, University of British Columbia Faculty of Medicine, Vancouver, BC, Canada; Vann Chau, The Hospital for Sick Children, Toronto, ON, Canada; Ruth Grunau, Unversity of British Columbia, Vancouver, BC, Canada; Steven P,.. Miller, University of British Columbia Faculty of Medicine, Vancouver, BC, Canada; Thiviya Selvanathan, University of British Columbia, Vancouver, BC, Canada
Post Doctoral Fellow University of British Columbia Vancouver, British Columbia, Canada
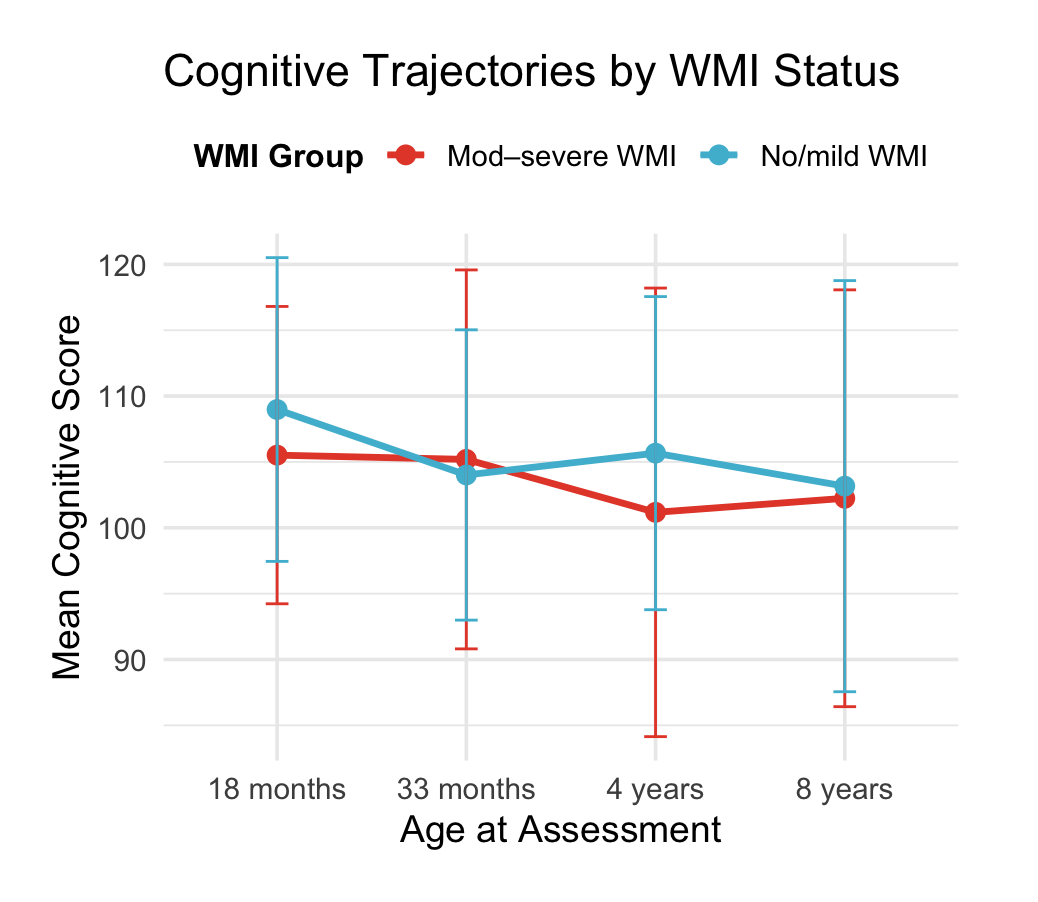
Background: Children born very preterm are at risk for enduring neurocognitive difficulties, including lower IQ and challenges in attention and executive functioning. While white matter injury (WMI) predicts poorer outcomes, children without moderate-severe WMI may also show later-emerging difficulties. Identifying neonatal risk factors for decline may guide targeted follow-up. Objective: To examine cognitive trajectories in very preterm children from 18 months to 8 years for children with and without moderate-severe WMI, and assess changes in low-IQ classification ( < 85) between 4 (WPPSI-III) and 8 years (WASI-II) and relationships with neonatal risk factors. Design/Methods: 234 infants born ≤32 weeks' gestation underwent neonatal MRI to characterize WMI. WMI was classified as no/mild ( < 40 mm³) or moderate-severe (≥40 mm³). Developmental assessments at 18, 33 months, 4.5, and 8 years used standardized measures (Bayley-III, WPPSI-III, WASI-II). McNemar's tests examined within-child change in IQ classification; Fisher's tests compared neonatal factors (ROP, CLD, NEC) between "declined" (≥85 to < 85) and "stable" (≥85 both) groups within the no/mild-WMI subgroup. Results: 130 children completed all follow-up visits. Cognitive trajectories varied by WMI status (Figure 1). The proportion scoring < 85 increased from 8% to 17%, χ²(1, N=128) =4.76, p=.03, significant only in those with no/mild WMI, χ²=5.06, p=.024. Among children with no/mild WMI, those who declined (n=13) had more CLD (38% vs 24%, p = .31), NEC (31% vs 16%, p = .24) compared to those who didn't, although not statistically significant. Over half of those in the declined group had ≥2 neonatal critical illnesses versus 42% of stable peers (p=.55). Children in the declined group were more often extremely preterm (54% vs 39%, p=.37).
Conclusion(s): Between 4 and 8 years, a higher proportion of preterm children fell below the low-IQ threshold, driven primarily by children with no/mild WMI on neonatal MRI. These findings suggest that children without significant brain injury may nonetheless experience subtle, progressive cognitive vulnerability as environmental and educational demands increase. While no neonatal factor independently predicted decline, trends linked greater prematurity, CLD, NEC and higher neonatal illness burden to later-emerging cognitive vulnerability, underscoring the need for ongoing monitoring and developmental support.
Figure 1: Cognitive Trajectories of Children from 18 months to 8 years by WMI status