513 - Low-dose obinutuzumab for the treatment of nephrotic syndrome in children
Saturday, April 25, 2026
3:30pm - 5:45pm ET
Publication Number: 2498.513
Megan A. Moravec, Cohen Children's Medical Center, Doylestown, PA, United States; Christine Sethna, Cohen Children's Medical Center, New Hyde Park, NY, United States; Krishna Daiya, Cohen Children's Medical Center, Queens, NY, United States
Clinical Pharmacy Specialist, Pediatric Nephrology and Solid Organ Transplant Cohen Children's Medical Center Doylestown, Pennsylvania, United States
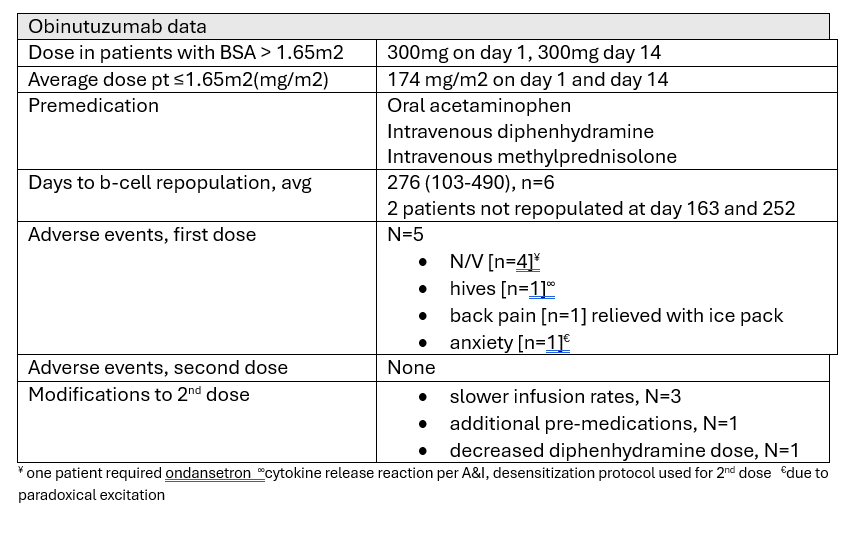
Background: Rituximab, a common anti-CD20 therapy for pediatric nephrotic syndrome (NS), faces challenges with resistance/intolerance. Obinutuzumab, a glycoengineered anti-CD20 antibody, shows promise in adults, but pediatric data is sparse. Objective: Evaluate low-dose obinutuzumab's safety and efficacy in pediatric NS, by assessing remission rates, duration of B-cell depletion, and adverse events (infusion reactions, neutropenia, hypogammaglobulinemia). Design/Methods: This retrospective chart review included children 0-18 years with NS receiving low-dose obinutuzumab (Jan 2024 - Mar 2025). Data collected includes demographics, dosing, premedications, infusion rates, adverse reactions, lab values (ie. CD19%, UPC), and remission status. Results: Seven children (average 12 years [3-15], 57% male) were included. Six (75%) had minimal change disease (MCD) and one (25%) had focal segmental glomerulosclerosis (FSGS). All had prior rituximab exposure, 2 (25%) had ofatumumab exposure. Patients received two doses as detailed in chart. No patients were in complete remission (CR) at baseline; 1 was in partial remission (UPC 1.3) and 6 were in relapse (UPC >2). All achieved B-cell depletion (CD19% < 1%) post-dose. CR was achieved in 5 patients (71.4%). Infusion-related reactions (IRRs) occurred in 5 patients (71.4%) during the first infusion (nausea/vomiting most common). All patients tolerated second infusions, often with modified protocols (slower infusion, additional premedication/desensitization, lower diphenhydramine dose). Of the 5 CR patients, 3 remained in CR with B-cells deplete or unchecked at last follow-up (Days 386, 163, 252). Average B-cell repopulation time in the 2 other patients was 343 days; both remained in CR at the time of repopulation. One patient received a second course of therapy due to B-cell repopulation (239 days post-obinutuzumab) while remaining in CR, and continued CR 302+ days post-second course. Two patients did not achieve remission; both had rapid B-cell repletion by days 103 and 138. One received only 75% of the first infusion due to an IRR. No hypogammaglobulinemia was observed when levels ordered. One patient presented to the ED between doses for unrelated reasons.
Conclusion(s): Low-dose obinutuzumab demonstrated favorable safety and efficacy, achieving high B-cell depletion and remission rates in pediatric NS. IRRs were common but manageable, with subsequent doses tolerated. These findings suggest low-dose obinutuzumab is a promising therapeutic option for pediatric NS patients intolerant to or not achieving remission with rituximab therapy. Further comparative studies are warranted.

 photo")