555 - Implementation of an Inclusive Decision Support Tool for Febrile Infants Age 7-90 Days in the Emergency Department
Saturday, April 25, 2026
3:30pm - 5:45pm ET
Publication Number: 2540.555
Dustin W. Ballard, Kaiser Permanente/CREST/UC Davis, San Anselmo, CA, United States; Madeline Somers, Kaiser Permanente Division of Research, Berkeley, CA, United States; David R. Vinson, The Permanente Medical Group, Orangevale, CA, United States; Tran Nguyen, Kaiser Permanente - Oakland Medical Center, Roseville, CA, United States; Margaret M. Stone, Kaiser Permanente Bernard J. Tyson School of Medicine, Los Anegels, CA, United States; Daniel D.. DiLena, Kaiser Permanente Division of Research, Pleasanton, CA, United States; Adina Rauchwerger, Kaiser Permanente, San Francisco, CA, United States; Tara L. Greenhow, Kaiser Permanente Northern California, San Francisco, San Francisco, CA, United States
Pediatric Infectious Diseases Kaiser Permanente Northern California, San Francisco San Francisco, California, United States
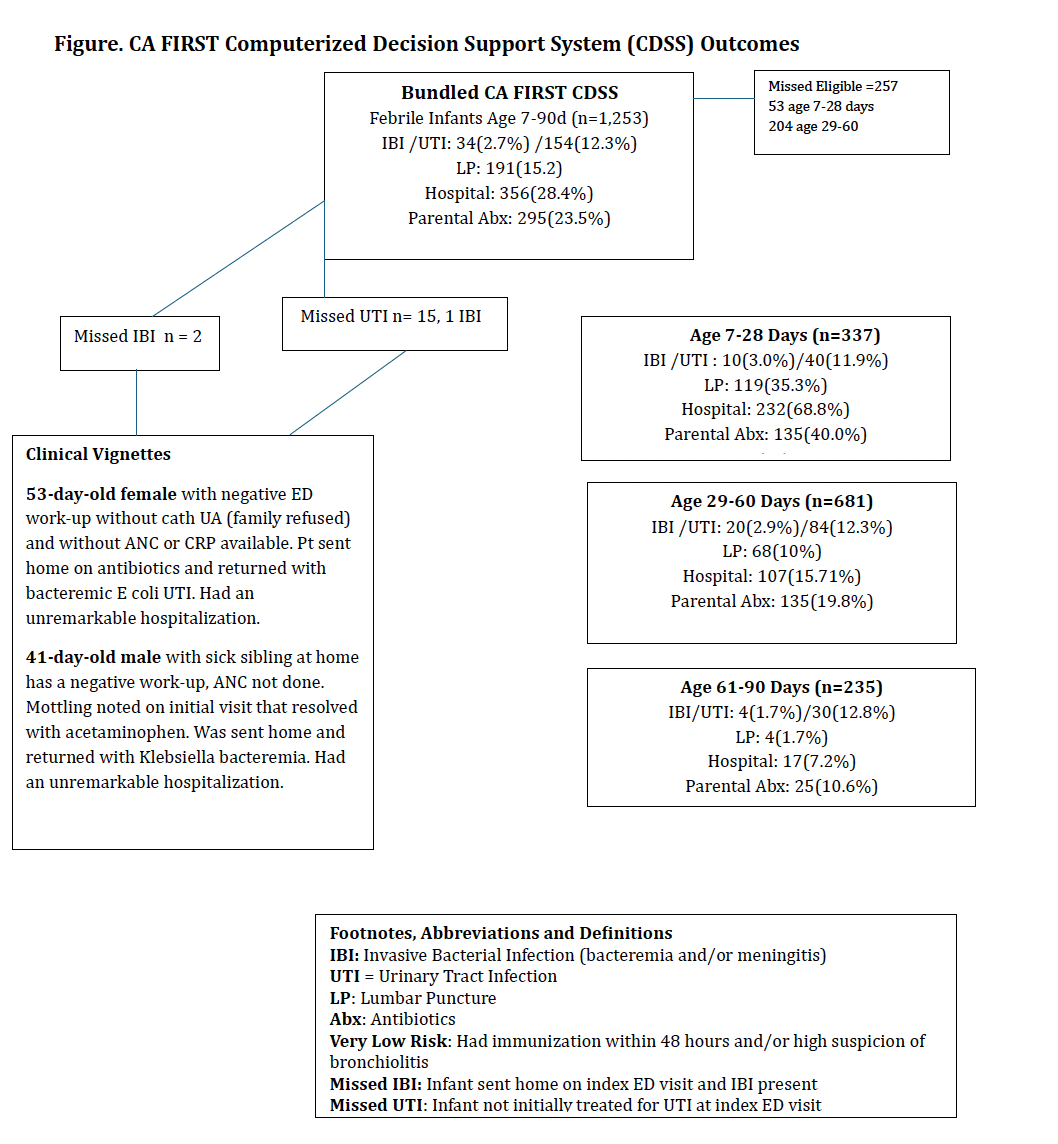
Background: Even with the recent publication of the American Academy of Pediatrics clinical practice guideline, the clinical approach to the febrile infant continues to evolve-providing an opportunity to test and deploy innovative tools that expand guidance and facilitate care. Objective: Within a large integrated healthcare delivery system, we aimed to evaluate enrollments in the California Febrile Infant Risk Stratification Tool (CA FIRST) computerized decision support system (CDSS) for febrile infants. Design/Methods: We conducted a retrospective evaluation of enrollments and outcomes for febrile infants aged 7-90 days in the CA FIRST CDSS, covering encounters from September 28, 2021, to December 31, 2024, across 21 Kaiser Permanente Northern California emergency departments (EDs). Infants were eligible if they had an ED chief complaint of fever or a measured temperature >38.0°C (100.4°F). The tool was accessed by the treating emergency and/or pediatric physician(s) and provided stepwise guidance both before and after laboratory investigation. Infants were excluded if they had a previous ED visit within 48 hours for fever evaluation or presented with signs or symptoms of septic shock. The CA FIRST CDSS captured clinical, laboratory, and physician gestalt data about febrile infants using standardized templates and definitions. High-risk past medical history attributes (e.g., prematurity) were pulled from the Epic-based electronic health record (EHR) (Table). Descriptive data were obtained from the CDSS records and supplemented with outcome data from the EHR. Results: A total of 1,253 infants were managed with CDSS guidance. Thirty-four (2.7%) were diagnosed with invasive bacterial infection, two of whom were discharged home after their index ED visit (Figure). Urinary tract infections (UTIs) were diagnosed in 154 infants (12.3%), including 15 with initially untreated UTIs identified on subsequent positive urine cultures. Overall, 15.2% (n=191) of infants underwent lumbar puncture (LP), 28.4% (n=356) were hospitalized, and 23.5% (n=295) received parenteral antibiotics at their index visit. The frequencies of LPs, hospitalizations, and parenteral antibiotic administration decreased with increasing age range (Figure).
Conclusion(s): Implementation of an integrated and comprehensive CDSS for febrile infants across EDs in a large California health system resulted in safe and effective management, with rates of LP and hospitalization within or below conventional parameters.

.jpg "Tara L. Greenhow, MD photo")
.png)