241 - Variability of Follow-up Skeletal Survey Completion in Child Physical Abuse: A Multicenter Study
Saturday, April 25, 2026
3:30pm - 5:45pm ET
Publication Number: 2232.241
Farah W.. Brink, Brink, Dublin, OH, United States; Tyler W. Ellis, Children's Hospitals and Clinics of Minnesota, Minneapolis, MN, United States; Sara Helwig, Nationwide Children's Hospital, Columbus, OH, United States; Charmaine B. Lo, Nationwide Children's Hospital, Columbus, OH, United States; Kendal L. Marston, Nationwide Children's Hospital, Powell, OH, United States; Loralie Peterson, University of Minnesota Masonic Children's Hospital, Minneapolis, MN, United States; Megan M.. Letson, Nationwide Children's Hospital, Columbus, OH, United States; Daniel M. Lindberg, University of Colorado Anschutz Medical Campus, Denver, CO, United States; Joanne Wood, Children's Hospital of Philadelphia, Philadelphia, PA, United States; Jan Leonard, CHOP, Philadelphia, PA, United States; M Katherine Henry, Children's Hospital of Philadelphia/UPenn, Philadelphia, PA, United States; James Anderst, Children's Mercy Hospitals and Clinics, Kansas City, MO, United States; Angela Bachim, Baylor College of Medicine, Houston, TX, United States; Kristine A. Campbell, University of Utah School of Medicine, Salt Lake City, UT, United States; Lori F. Frasier, Penn State Hershey, Hershey, PA, United States; Natalie Laub, University of California, San Diego School of Medicine, San Diego, CA, United States; Margaret Russell, UPMC Childrens Hospital of Pittsburgh, Pittsburgh, PA, United States; Nancy S. Harper, University of Minnesota Masonic Children's Hospital, Minneapolis, MN, United States
Assistant Professor Nationwide Children's Hospital Columbus, Ohio, United States
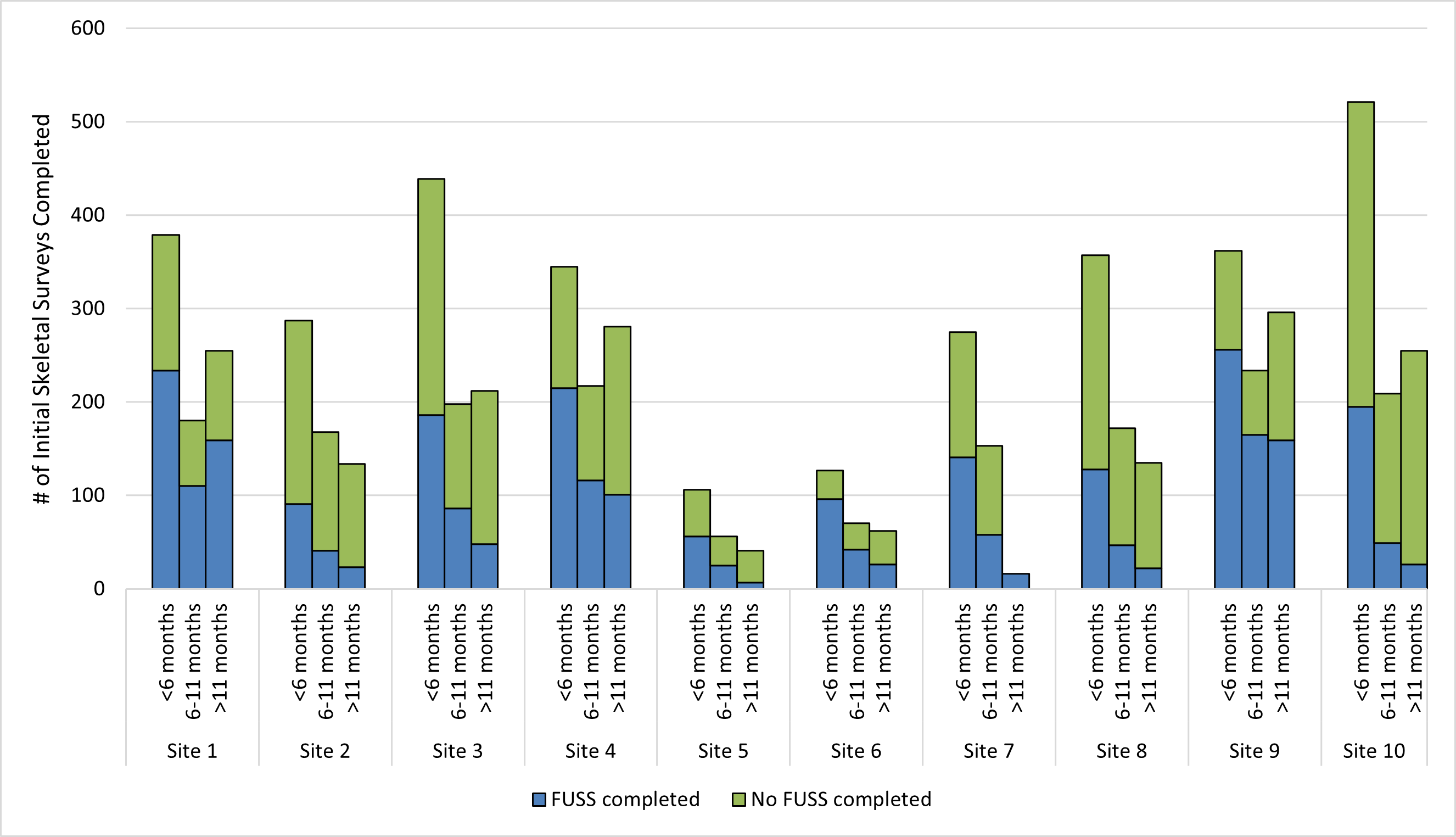
Background: Children < 2 years are at risk for abusive fractures. A skeletal survey (SS) is recommended when abuse is suspected and then repeated in 2 weeks. Although follow-up skeletal surveys (FUSS) can often identify new information, completion rates are highly variable. Objective: To determine rates and variability of FUSS completion for children who received an initial SS within a multi-site child abuse research network and identify characteristics associated with FUSS completion. Design/Methods: This was a retrospective study of children < 2 years who had an initial SS during evaluation of possible physical abuse by a child abuse practitioner (CAP) from 2/1/2021-4/30/24 across 10 sites contributing data to CAPNET. Independent variables included age, initial SS findings (identifies/raises concern for fracture), level of concern (LOC) for abuse (1-3 vs 4-7), and concerning injuries. The dependent variable was proportion of FUSS completion. Concerning injuries were defined as specific fractures (e.g., rib fractures), TEN-4-FACEs bruising, specific intracranial injuries (e.g., subdural hemorrhage with characteristic retinal hemorrhages), and intraabdominal injuries. Descriptive statistics summarized patient demographics and characterized FUSS completion for the study population and stratified by age ( < 6 months old vs >=6 to < 11 months old vs >=11 to < 24 months old), initial SS findings, and LOC for abuse. Two multiple logistic regression models were used to characterize FUSS as a function of age, initial SS findings, and LOC for abuse. A model with a random effect for site was compared to a model without a random effect for site, using a likelihood ratio test. A confidence level of 95% was used throughout, and confidence intervals were reported whenever possible. Results: Of 12,096 eligible CAPNET encounters, 6631 encounters of 6514 unique patients met inclusion criteria. Most were < 6 months old (48.2%), male (57.8%), non-Hispanic white (44.4%), and had public insurance/no insurance/self-pay (73.9%) (Table 1). Overall, FUSS was completed in 44.1% of encounters. Completion of FUSS was associated with high LOC (aOR 7.0, 95% CI 6.1-8.0), presence of fracture on initial SS (aOR 2.8, 95% CI 2.4-3.1), and concerning injury (aOR 2.2, 95% CI1.9-2.5). Despite controlling for all variables, significant variation between sites of FUSS completion was observed (26.3%-65.0%, p< 0.001) (Fig 1).
Conclusion(s): In conclusion, patient characteristics and site contribute to significant variability in FUSS completion among children evaluated by CAPs with an initial SS.
Table 1. Demographics of patient encounters across CAPNET sites and by FUSS completion.
Figure 1. Distribution of FUSS completion across CAPNET stratified by age and site.

 photo")
.jpg)