Session: Neonatal Hematology & Transfusion Medicine 1
154 - Enteral Feeding Practices Around Neonatal PRBC Transfusion in the United States
Saturday, April 25, 2026
3:30pm - 5:45pm ET
Publication Number: 2148.154
Irfan Shehzad, Pediatrix Neonatology of San Antonio, Boerne, TX, United States; Kelsey Coombs, West Virginia University Children's Hospital, Morgantown, WV, United States; Lesley A. Cottrell, West Virginia University, Morgantown, WV, United States; Mahmoud Ali, West Virginia University Children's Hospital, Morgantown, WV, United States
Pediatrix Neonatology of San Antonio Boerne, Texas, United States
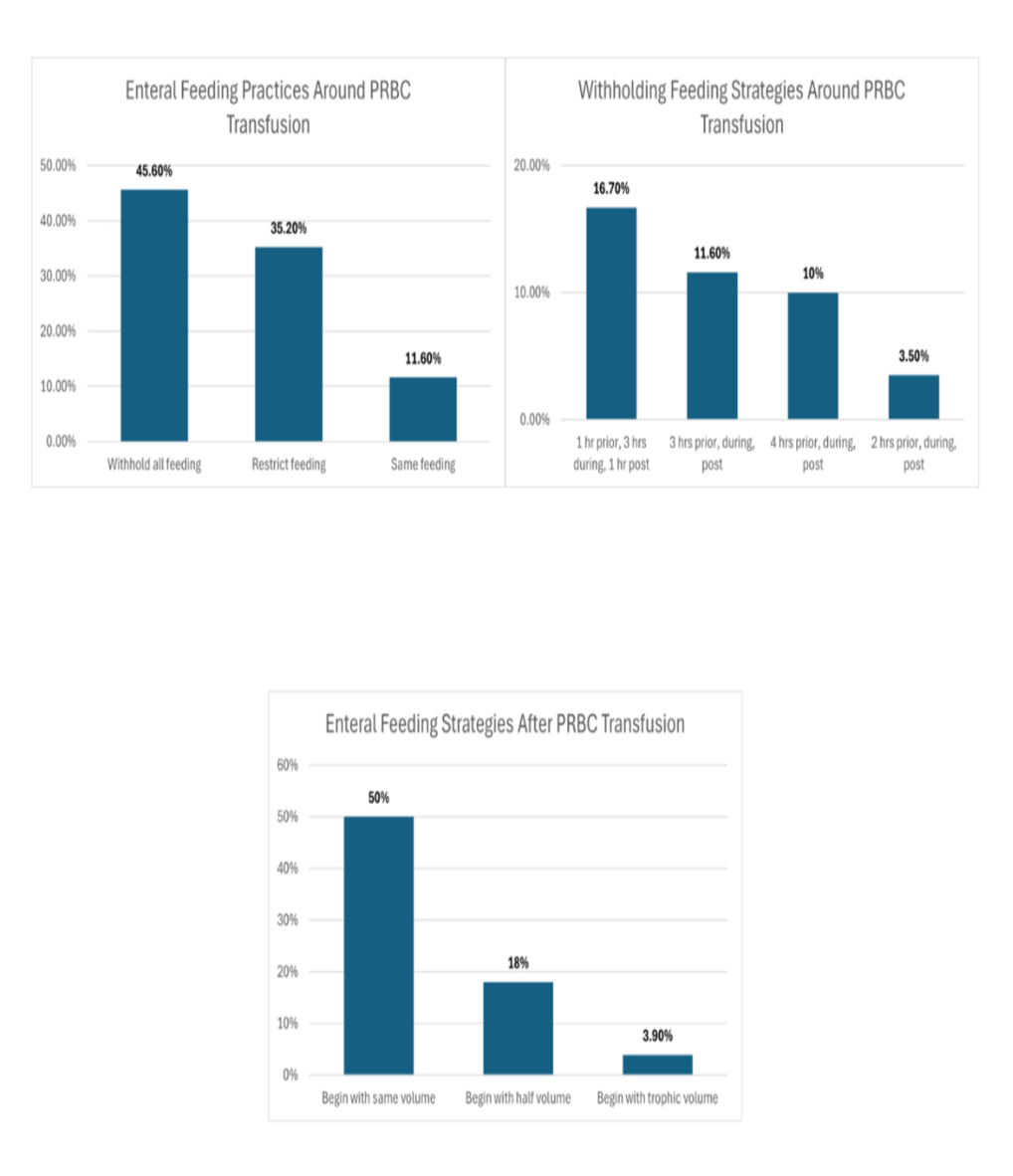
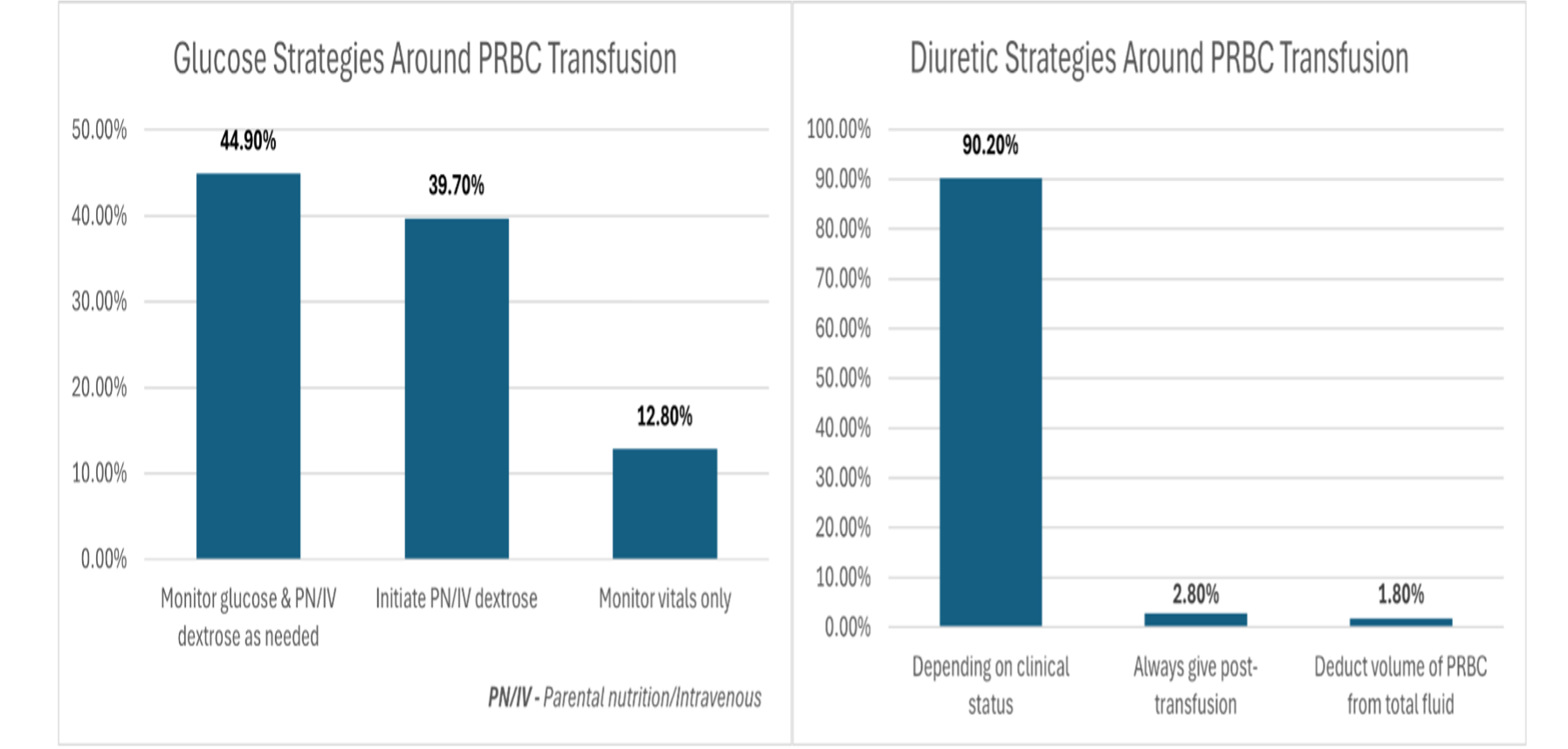
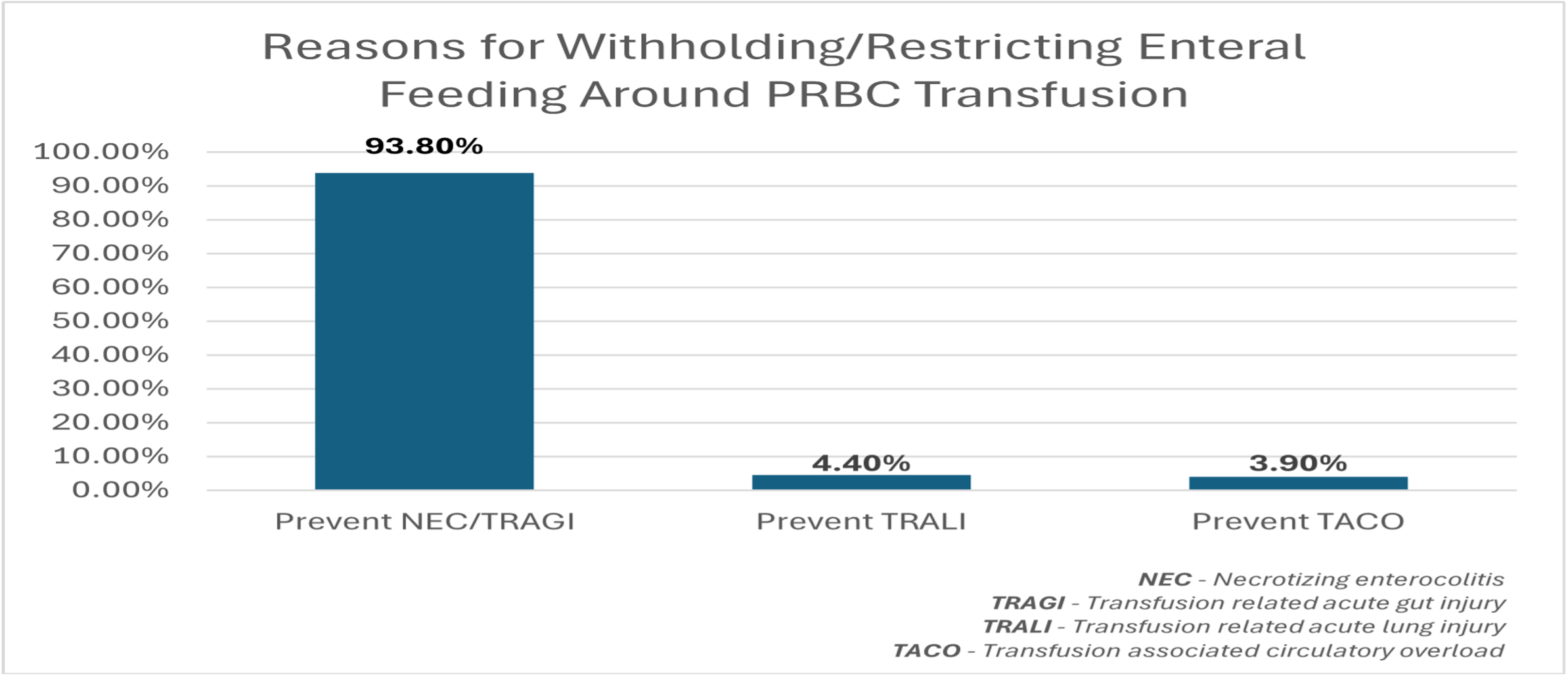
Background: Infants in neonatal intensive care units (NICUs) are at high risk for anemia requiring packed red blood cell (PRBC) transfusion. Factors such as erythrocyte transfusion, enteral feeding, and gastrointestinal immaturity have been implicated in necrotizing enterocolitis (NEC) or Transfusion-related acute gut injury (TR-AGI), with conflicting evidence. Despite these concerns, there is no standardized protocol guiding enteral feeding around PRBC transfusion in the NICU and practice varies widely among providers. Objective: We aimed to assess current opinions and enteral feeding practices around PRBC transfusion among NICU providers in the United States. Design/Methods: A REDCap (Research Electronic Data Capture) survey consisting of 10 questions was distributed to members of the Section on Neonatal-Perinatal Medicine (SoNPM) and the Trainees and Early Career Neonatologists (TECaN) groups of the American Academy of Pediatrics (AAP). Descriptive statistics were used to analyze responses. Results: A total of 425 providers completed the survey. Nearly (80%) were neonatologists at various career stages. More than half (59.5%) reported that their NICU has a feeding guideline related to PRBC transfusion. Approximately (45.6%) withhold all enteral feeds, (35.2%) restrict feeds and (11.6%) continue feeds unchanged. Among those withholding feeds, (16.7%) stop feeding entirely for a defined period, with the most common intervals being 1-hour pre-transfusion, 3-hours during, and 1-hour post-transfusion. When resuming feeds, (50%) restart at the same volume and method as before; (18%) begin with half volumes and advance as tolerated. (Figure 1). Small proportion (37.3%) indicated the presence of an institutional protocol for monitoring glucose levels during transfusion. Regarding diuretic use post transfusion, (90.2%) indicated that diuretic administration depends on patient's clinical status. (Figure 2). A majority (93.8%) identified the NEC/AGI are the primary reasons for withholding or restricting enteral feeds around transfusion (Figure 3).
Conclusion(s): Most NICUs either withhold or restrict enteral feeding around PRBC transfusion, although approaches remain highly variable. Despite inconsistent evidence regarding the impact of enteral feeding on transfusion-related gut complications, concern for NEC/TR-AGI remains prevalent among providers. These findings highlight the need for multicenter clinical trials to develop an evidence-based, safe and consensus driven enteral feeding protocol for neonates receiving PRBC transfusion.