488 - The Association of Puberty and Compensatory Hypertrophy on Kidney Function in Pediatric Patients with Congenital Solitary Functioning Kidney
Saturday, April 25, 2026
3:30pm - 5:45pm ET
Publication Number: 2475.488
Hannah Bender, University of Washington School of Medicine, Seattle, WA, United States; Sangeeta Hingorani, University of Washington School of Medicine/Seattle Children's Hospital, Seattle, WA, United States; Jinqiu Du, University of Washington, Seattle, WA, United States
Medical Student University of Washington School of Medicine Seattle, Washington, United States
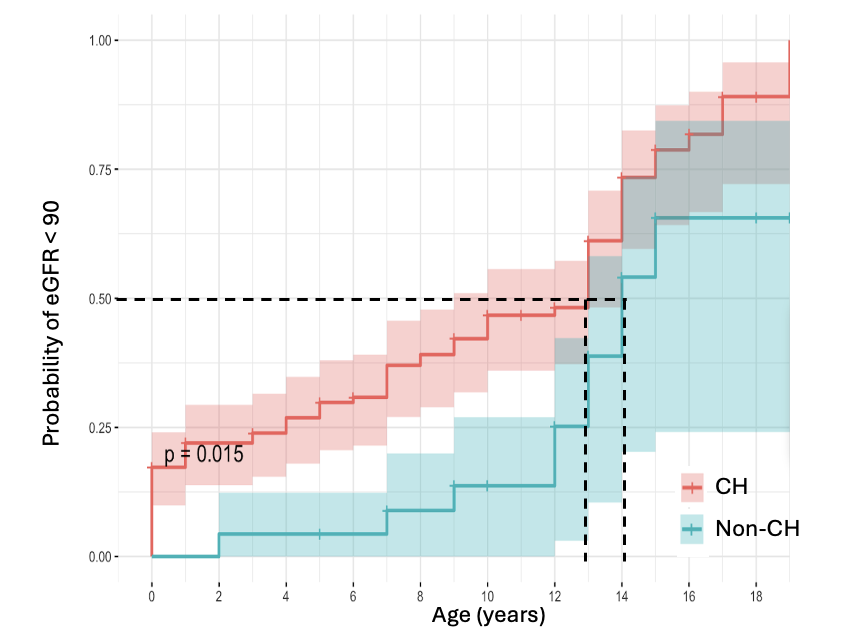
Background: Congenital solitary functioning kidney (cSFK), in which an individual is born with only one anatomical or functional kidney, is a known risk factor for chronic kidney disease (CKD) and includes diagnoses such as multicystic dysplastic kidney (MCDK) and unilateral renal agenesis (URA). While animal studies suggest that compensatory hypertrophy (CH) may be protective by increasing nephron size, recent evidence indicates it may instead promote hyperfiltration, which over time leads to scarring, and nephron loss. Kidney function decline has been associated with puberty, though mechanisms remain unclear. Objective: We aimed to assess whether puberty contributes to reduced kidney function and albuminuria in pediatric cSFK, and whether CH affects long-term outcomes. Design/Methods: We conducted a retrospective cohort study of 170 pediatric cSFK patients aged 8-20 years treated at Seattle Children's Hospital (2015-2024). Primary outcomes were eGFR, albuminuria, and blood pressure (BP). eGFR was calculated using the Schwartz equation. Albuminuria was defined as urine albumin-to-creatinine ratio >30 mg/g. Hypertension followed 2017 AAP criteria (>95th percentile by age, sex, height). Exposure groups were pubertal status (pre- vs. post-pubertal) and presence of CH. Kaplan-Meier curves evaluated time to eGFR < 90. Longitudinal associations of CH, puberty, and outcomes were assessed using mixed-effects models adjusted for diagnosis, kidney location, and sex. The study protocol has IRB approval. Results: Patients with CH had on average +8.9 mL/min/1.73m² higher eGFR than those without CH (95%Cl[5.1-12.7], p=0.021). Kaplan-Meier analysis demonstrated that patients with CH had a significantly greater cumulative probability of developing reduced kidney function (eGFR < 90) over time compared to those without CH (p = 0.015). CH was associated with elevated systolic BP +1.9 mmHg (95%CI[0.9-2.9], p< 0.05), but not diastolic BP or albuminuria. After adjusting for CH, puberty was associated with ~2-folds increased odds of developing an eGFR < 90 (OR=1.83, p=0.02) compared to pre-pubertal patients. Puberty was associated with an increase in systolic BP +9.1 mmHg (95%CI[7.9-10.3], p< 0.001) and diastolic BP +3.9 mmHg (95%CI[3-5.1], p< 0.001).
Conclusion(s): In pediatric cSFK, CH is associated with initially preserved kidney function but a more rapid decline in eGFR over time. Puberty is independently associated with increased health risk, with higher odds of eGFR decline and a rise in systolic BP. These findings highlight the importance of longitudinal monitoring of renal function and BP in cSFK, particularly through adolescence.
Demographic and Clinical Features of 170 Children with cSFK
Cumulative Probability of Reduced Kidney Function (eGFR <90) in Patients with CH vs Patients without CH

 photo")
.png)