481 - Major Adverse Kidney Events in Children and Young Adults with Acute Kidney Injury: A PEDSNET Study
Saturday, April 25, 2026
3:30pm - 5:45pm ET
Publication Number: 2469.481
Shina Menon, Stanford University School of Medicine, Palo Alto, CA, United States; Katja Gist, University of Colorado School of Medicine, Aurora, CO, United States; Christine Cunningham, Stanford University School of Medicine, Palo Alto, CA, United States; Bren Botzheim, Stanford University School of Medicine, Oakland, CA, United States; Nymisha Chilukuri, Stanford University School of Medicine, San Francisco, CA, United States; Victor Ritter, Stanford University School of Medicine, Palo Alto, CA, United States; Scott Sutherland, Stanford University School of Medicine, Palo Alto, CA, United States
Stanford University School of Medicine Palo Alto, California, United States
Background: Acute Kidney Injury (AKI) is a common and serious complication in children and young adults admitted to the intensive care unit (ICU), associated with increased morbidity and mortality. While short-term outcomes are well-documented, data regarding clinically relevant long-term adverse kidney outcomes in this population remain scarce, especially across diverse, large-scale cohorts in the United States. Objective: To quantify the incidence of Major Adverse Kidney Events at 90 days and 365 days (MAKE-90 and MAKE-365) in children and young adults experiencing AKI in the ICU using the large, federated PEDSNET electronic health record (EHR) database. Design/Methods: This was a retrospective cohort study utilizing data from the PEDSNET research network. Inclusion criteria were age 3 months to 25 years; admitted for more than 2 days in the ICU between 2014-2024; > 1 serum creatinine (SCr) during hospital stay. Exclusion criteria were presence of CKD stage 4 or 5, receipt of chronic dialysis or kidney transplant prior to index admission. AKI was defined using Kidney Disease: Improving Global Outcomes (KDIGO) criteria. Baseline SCr was defined as the median of values between 7 and 365 days before admission. In those with no previous SCr available, baseline SCr was imputed using age, sex based normative values as recommended by PODIUM guidelines. The primary outcomes were MAKE-90 and MAKE-365, a composite endpoint defined as the occurrence of: (1) death; (2) initiation of new renal replacement therapy (RRT); or (3) persistent kidney dysfunction (> 25% decline in estimated glomerular filtration rate (eGFR) from baseline at 90 days and 365 days respectively. Results: A total of 103362 patients were included in the final cohort of which baseline SCr was available for 38618 (37%) and 17731 (17.1%) had AKI (Table 1). The overall incidence of MAKE-90 in those with AKI was 21% and in those without AKI was 3.7%, and the incidence of MAKE-365 in those with AKI was 26% compared to 6.3% in those without AKI (Table 2). Dialysis dependence at 90 days after an episode of AKI was seen in 1.5%. Incidence of MAKE-90 increased with AKI stage (12% in those with AKI stage 1, 20% in AKI stage 2 and 39% in AKI stage 3).
Conclusion(s): MAKE-90 is a common and important outcome in children and young adults following AKI. The high incidence of MAKE-90 highlights the need for dedicated follow-up care and targeted interventions in high-risk groups, specifically those with. Next we plan to look at the risk factors for MAKE 90 and MAKE 365 within this dataset.
Table 1 Baseline Characteristics of the Cohort
Table 2 Incidence of MAKE and its component outcomes

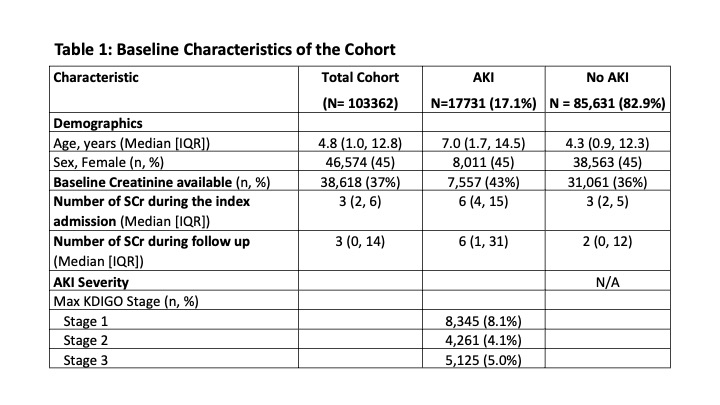 Baseline Characteristics of the Cohort
Baseline Characteristics of the Cohort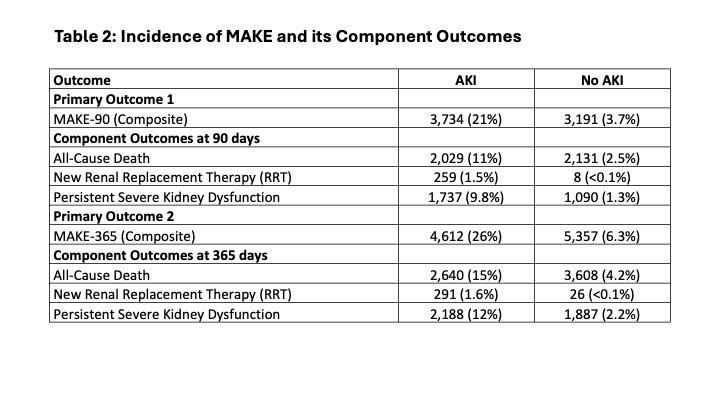 Incidence of MAKE and its component outcomes
Incidence of MAKE and its component outcomes