554 - Febrile Young Infant Evaluation in the Community Emergency Department Before and After Implementation of an Institutional Guideline
Saturday, April 25, 2026
3:30pm - 5:45pm ET
Publication Number: 2539.554
Catherine E. McCarthy, Janet Weis Children's Hospital at Geisinger, Danville, PA, United States; Andrea Berger, Geisinger, Danville, PA, United States; Brad M. Rickabaugh, Geisinger Medical Center, Danville, PA, United States; Nancy Clemens, Janet Weis Children's Hospital at Geisinger, Danville, PA, United States
Resident Physician Janet Weis Children's Hospital at Geisinger Danville, Pennsylvania, United States
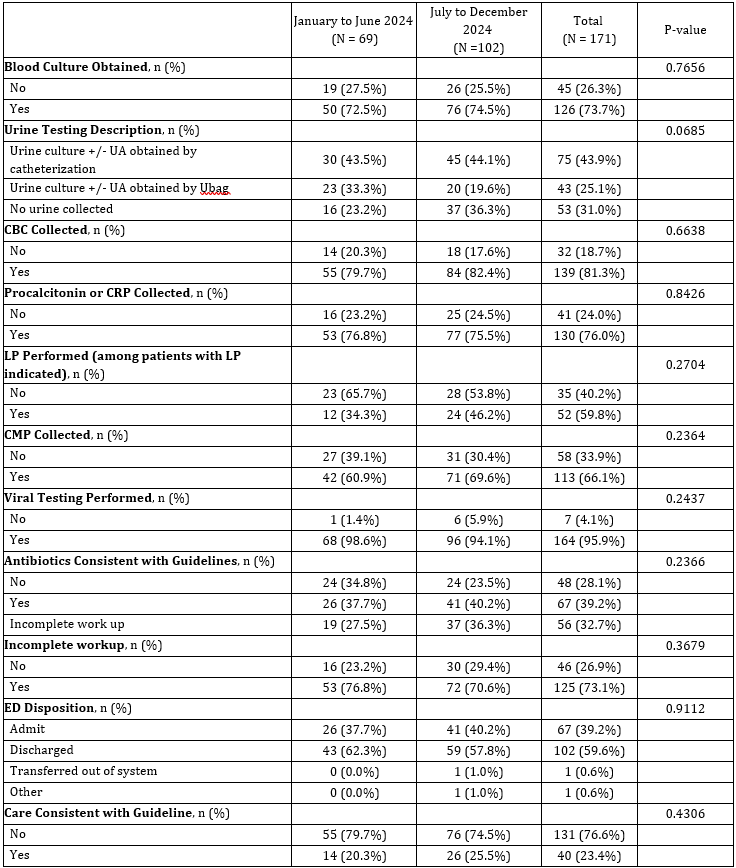
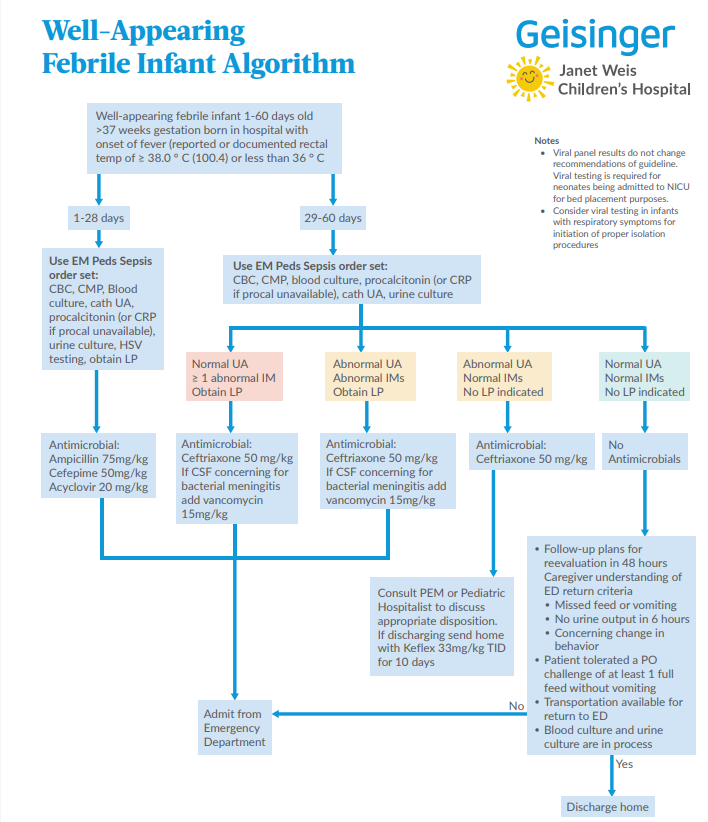
Background: The American Academy of Pediatrics released updated guidelines for managing well-appearing febrile infants in 2021. Most infants, however, receive emergency care in community emergency departments (EDs) from clinicians without pediatric specialty training. Evaluation outside children's hospitals remains poorly described. The Geisinger Health System (GHS), a rural network with nine community EDs, developed and implemented a simplified electronic health record (EHR)-based guideline to standardize care for this population (Figure 1). Objective: Compare evaluation and treatment of febrile infants ≤60 days old before and after implementation of an EHR-based guideline. Design/Methods: Retrospective chart review of infants ≤60 days presenting to all GHS EDs from January 1 to December 31, 2024, with fever ≥100.4°F at home or in the ED. Patient demographic and evaluation data were abstracted. Urine testing was categorized as (1) urine culture +/- urinalysis (UA) obtained by catheterization (2) urine culture +/- UA obtained by Ubag or (3) no urine obtained. A complete evaluation required blood culture, CBC, procalcitonin or C-reactive protein, comprehensive metabolic panel, and catheterized UA with culture. Guideline adherence with antibiotic use and lumbar puncture was assessed. Data were compared before and after implementation using descriptive statistics and chi-square testing. Results: Among 1,316 encounters, 171 met inclusion criteria (69 pre-guideline [40.4%], 102 post-guideline [59.6%]) (Table 1). Three of the nine GHS EDs evaluated ≤ 5 febrile neonates during the study period. Workups were incomplete in 76.8% of pre-guideline and 70.6% of post-guideline cases (p=0.37)(Table 2). Care consistent with the guideline rose from 20.3% to 25.5% post-implementation, though not statistically significant (p=0.43). Fewer than half of infants received recommended urine testing, while viral testing was performed in over 95% of cases.
Conclusion(s): The preliminary data demonstrates a minority of febrile neonates received recommended care in the community setting. Easy access to an EHR-based guideline modestly improved adherence but did not achieve statistical significance. Gaps in urine testing highlight opportunities for provider education and system-level interventions. Utilization of standardized electronic tools may support pediatric readiness and promote consistent, evidence-based care across community EDs.
Figure 1. Geisinger Health System Well-Appearing Febrile Infant Guideline

 photo")
.png)