Session: Neonatal Hematology & Transfusion Medicine 1
162 - Cryoprecipitate utilization in the neonatal intensive care unit: a single-center experience
Saturday, April 25, 2026
3:30pm - 5:45pm ET
Publication Number: 2156.162
Ashley Stoeckel, Boston Children's Hospital, Boston, MA, United States; Erin Soule-Albridge, Boston Children's Hospital, Boston, MA, United States; Henry A.. Feldman, Boston Children's Hospital, Boston, MA, United States; Martha Sola-Visner, Harvard Medical School, Boston, MA, United States; Patricia Davenport, Boston Children's Hospital, Boston, MA, United States
Pediatric Surgery Research Fellow Boston Children's Hospital Boston, Massachusetts, United States
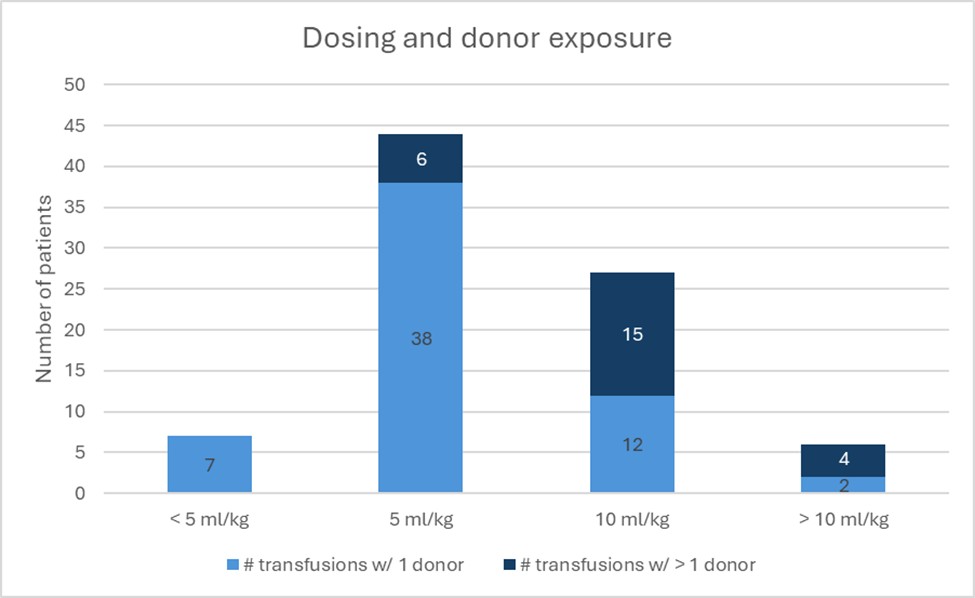
Background: Despite advancements in neonatal transfusion medicine, the majority of centers do not have clinical guidelines for cryoprecipitate transfusion in neonates. This results in significant variability in both the fibrinogen threshold used for transfusion and in the dosing of cryoprecipitate. Higher doses can result in the exposure of neonates to multiple donors after a single transfusion, which is associated with transfusion-related complications. A recent study showed that limiting the cryoprecipitate transfusion volume to a single unit (20-25mL) in neonates did not negatively impact the efficacy of the transfusion (defined as achieving a fibrinogen level over 150mg/dL) and limited the exposure to a single donor. Objective: In this study, we investigated the cryoprecipitate transfusion practices in our level IV neonatal intensive care unit (NICU). Design/Methods: In this retrospective study, all cryoprecipitate transfusions administered to infants admitted to our Hospital's NICU from January 2022 through December 2024 were reviewed. Patient characteristics, diagnoses, fibrinogen levels and transfusion indications were collected through chart review. Results: 50 patients received 104 cryoprecipitate transfusions. The majority of patients were admitted with a surgical diagnosis, of which 44% had either necrotizing enterocolitis (NEC) or spontaneous intestinal perforation (SIP). The median fibrinogen level prompting transfusion was 100 mL/dL (range < 15-586) and the majority of transfusions were ordered at either 5 mL/kg (n=37) or 10 mL/kg (n=22), and resulted in a median post-transfusion increase in fibrinogen of 81 mg/dL or 142 mg/dL, respectively. The median post-transfusion fibrinogen level for all transfusions was 212 mL/dL (range 65-592 mL/dL), with 75% of 5mL/kg transfusions and 91% of 10mL/kg transfusions achieving a post-transfusion fibrinogen level > 150 mL/dL. Overall, 11% of 5mL/kg and 48% of 10mL/kg transfusions likely resulted in multiple donor exposure (Figure 1).
Conclusion(s): There is significant variation in cryoprecipitate transfusion practices, even within a single center. While higher doses resulted in a greater increase in the post-transfusion fibrinogen level, achieving a post-transfusion fibrinogen level over 150mL/dL 91% of the time, it also resulted in a higher likelihood of exposure to multiple donors. More research is needed to better understand the risk/benefit of cryoprecipitate dosing in order to develop and implement evidenced based guidelines to both effectively care for critically ill neonates while also limiting donor exposure to prevent additional harm.
Figure 1. Weight-based dosing per cryoprecipitate transfusion given with anticipated donor exposure.

 photo")