549 - Bacteremia Outcomes After Initial discharge from the Emergency Department; A Ten-Year Single Center Retrospective Analysis
Saturday, April 25, 2026
3:30pm - 5:45pm ET
Publication Number: 2534.549
Stephen Rineer, University of Colorado School of Medicine, Aurora, CO, United States; Halden F. Scott, University of Colorado School of Medicine, Denver, CO, United States; Mairead Dillon, University of Colorado School of Medicine, Denver, CO, United States
Assistant Professor of Pediatrics University of Colorado School of Medicine Aurora, Colorado, United States
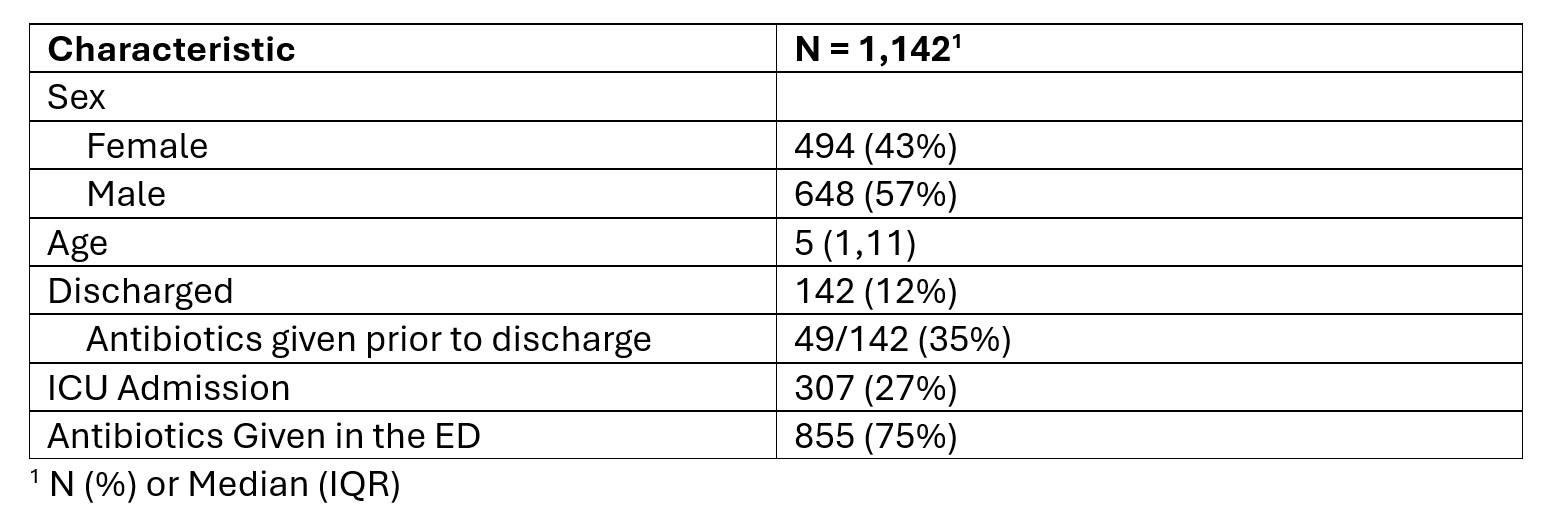
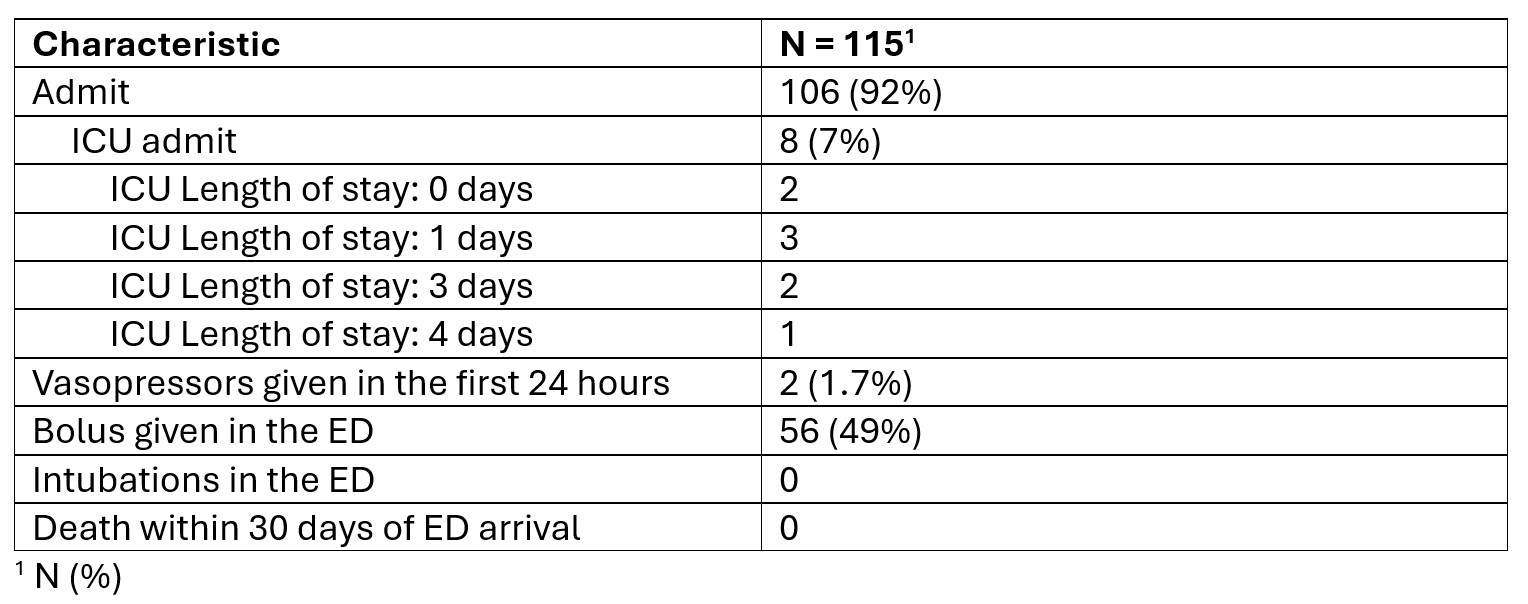
Background: Bacteremia is a rare but rising threat to child health through declining vaccination rates and emerging invasive pathogens like group A strep (iGAS). The cost of missed diagnoses can be as severe as the preventable death of a child. An estimated 7000 children die per year in the USA from bacteremia progressing to sepsis. Limited data is available on outcomes of children discharged from the emergency department (ED) after blood culture collection. Objective: Evaluate outcomes for children discharged from the ED after blood culture collection with subsequent positive blood culture result. Design/Methods: This retrospective single center study utilized a pre-existing mapped registry of children 0-18 years old, including all visits to the ED with a blood culture obtained from January 2014 to December 2024. This study was IRB exempt. The registry comprised 53,143 unique individual encounters and 1,142 positive blood cultures. Positive blood culture organism data was cross referenced with CDC commensal organism list and expert review to eliminate contaminant blood culture results. Children with positive blood cultures were stratified by disposition. Discharged children were assessed for outcomes upon return to the ED within 72 hours post-initial discharge including disposition, ICU length of stay, vasoactive support, fluid boluses given and death at 30 days. Results: In our cohort, 142 children out of 1,142 (12%) were discharged from the ED after blood culture collection with a subsequent positive result (table 1). Of these 142, 49 (35%) received antibiotics in the ED prior to discharge (table 1). 115 children returned to the ED within 72 hours and 106 (92%) were admitted to our institution. Only 8 children (7%) required intensive care (ICU). 2 of these children required less than 24 hours of ICU care. 2 children (1.7%) required vasoactive support, and no ED intubations were recorded. 56 (49%) were given a fluid bolus in the ED. No deaths were reported from this population in 30 days.
Conclusion(s): Discharge from the ED is common after blood culture collection. Clinical deterioration is rare as evident by few children requiring vasoactive support, intubation or ICU admission from this population. No deaths were evident in our cohort through ten years of retrospective data. While this event remains rare, more studies are required to better risk stratify this at-risk population.