84 - Sequential Introduction of Maternal RSV Vaccination and Infant Nirsevimab Immunization: Early Real-World Experience from an Urban Bronx Cohort
Saturday, April 25, 2026
3:30pm - 5:45pm ET
Publication Number: 2080.84
Edward Lopez, BronxCare Health System, White plains, NY, United States; Mohamed Ghamry, BronxCare Health System, Bronx, NY, United States; Savita Manwani, Bronx Care Health System, Bronx, NY, United States; Emmy Kristine Trinidad, BronxCare Health System, Bronx, NY, United States; Merve Arslan Aydin, BronxCare Health System, Bronx, NY, United States; Nestor Trujillo, Bronx Care Health System, Bronx, NY, United States; Charles Ch. Ihedioha, bronx-lebanon, Bronx, NY, United States; Pratibha Ankola, Icahn School of Medicine at Mount Sinai, Bronx, NY, United States
Pediatric Resident BronxCare Health System White plains, New York, United States
Background: Maternal RSVpreF vaccination and infant nirsevimab immunization were introduced sequentially in the U.S.-nirsevimab for high-risk infants in 2023-2024 and both maternal and universal infant programs in 2024-2025. Data on early real-world impact in underserved populations remain limited. Objective: To assess the early effect of maternal RSV vaccination and infant nirsevimab on RSV infection, hospitalization, and respiratory outcomes during the transition from targeted to universal implementation. Design/Methods: We conducted a retrospective cohort of 949 infants born October 2023-December 2024 at BronxCare Health System. During 2023-2024, nirsevimab was limited to high-risk infants; by 2024-2025, both programs were available. Outcomes included RSV infection, bronchiolitis, RSV-related hospitalization, and respiratory support. Analyses used χ² and multivariable logistic regression adjusting for gestational age ( < 37 weeks), maternal age ≥35 years (AMA), race/ethnicity, and season. Results: Among 949 infants, 38 (4.0%) developed RSV. Immunization coverage increased from 27.1% in 2023-2024 to 32.7% in 2024-2025 (p=0.075). RSV occurred in 3.8% of immunized vs 4.1% of unimmunized (p=0.82) and 2.4% of infants born to vaccinated vs 4.1% of unvaccinated mothers (p=0.58). Adjusted models showed no significant associations for infant immunization (aOR 1.38; 95% CI 0.53-3.59) or maternal vaccination (aOR 0.85; 95% CI 0.13-5.47). RSV-related hospitalizations occurred in 1.9%; both ward (1.7% vs 0.6%) and PICU (0.6% vs 0.3%) admissions were higher among unimmunized (p=0.31). Respiratory support was needed in 1.9%, with none of the immunized requiring invasive ventilation. Findings were consistent for bronchiolitis (aOR 1.10; p=0.76).
Conclusion(s): This analysis captures the transition from targeted to universal RSV-prevention in an urban cohort. RSV infection, bronchiolitis, and RSV-related hospitalization were numerically lower among immunized infants and those born to vaccinated mothers, though not significant, likely reflecting limited early adoption and low incidence during rollout. Severity outcomes-including ward, PICU admission, and respiratory support-were all higher in unimmunized infants, suggesting a potential protective trend requiring confirmation in multi-season studies.
Table 1 Demographic Characteristics of Study Participants (n = 949)


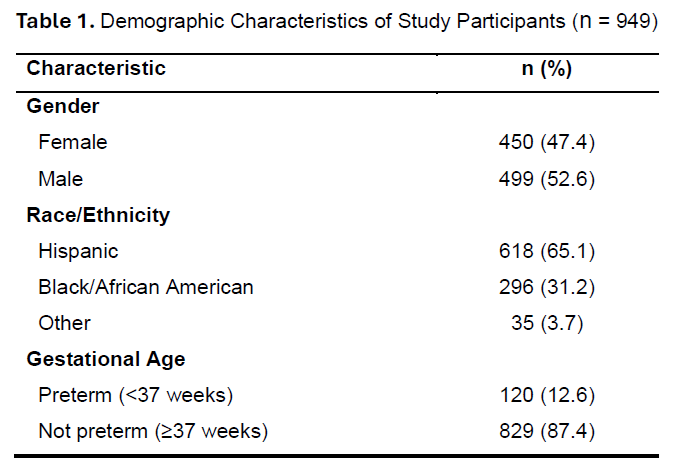 Demographic Characteristics of Study Participants (n = 949)
Demographic Characteristics of Study Participants (n = 949)