317 - Development and Internal Validation of a Model to Predict Hospitalization for Children with Asthma Exacerbations in the Emergency Department
Saturday, April 25, 2026
3:30pm - 5:45pm ET
Publication Number: 2306.317
Melisa Tanverdi, University of Colorado School of Medicine, Aurora, CO, United States; Mairead Dillon, University of Colorado School of Medicine, Denver, CO, United States; John Brinton, University, Aurora, CO, United States; Iriam J. Islas, University of Colorado School of Medicine, Denver, CO, United States; Christopher Linn, University of Colorado School of Medicine, Aurora, CO, United States; Cesar I. Romero Carreon, Children's Hospital Colorado, Aurora, CO, United States; Rebecca Helmuth, University of Colorado School of Medicine, Parker, CO, United States; Rakesh D. Mistry, Yale School of Medicine, New Haven, CT, United States; Max A.. Seibold, National Jewish Health, Denver, CO, United States; Stanley J. Szefler, University of Colorado School of Medicine, Aurora, CO, United States; Andrew H. Liu, Children's Hospital Colorado, Aurora, CO, United States; Katharine L. Hamlington, University of Colorado Anschutz, Aurora, CO, United States; Todd A. Florin, Ann & Robert H. Lurie Children's Hospital of Chicago, Chicago, IL, United States; Nidhya Navanandan, University of Colorado School of Medicine, Aurora, CO, United States
Assistant Professor University of Colorado School of Medicine University of Colorado School of Medicine Aurora, Colorado, United States
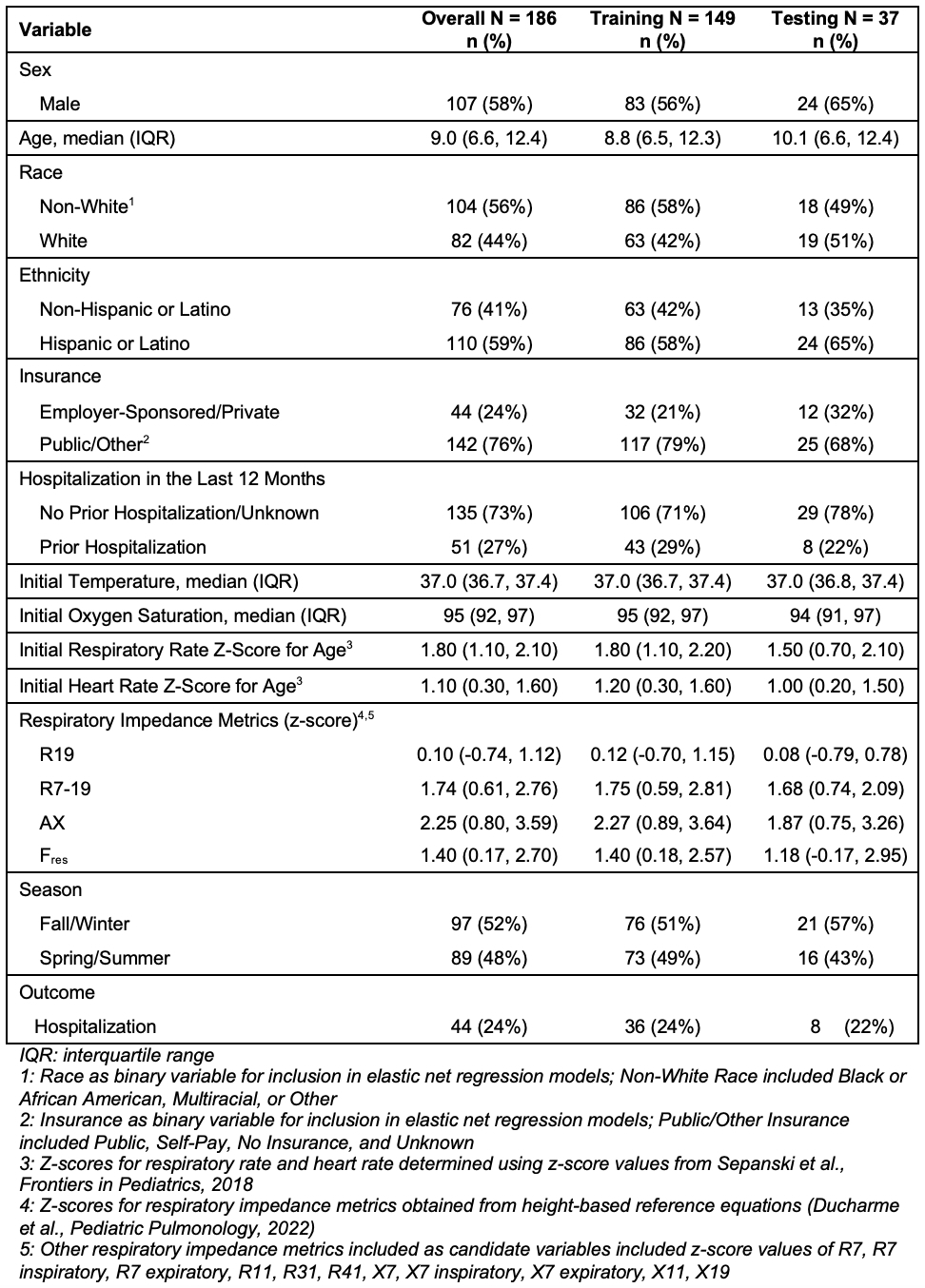
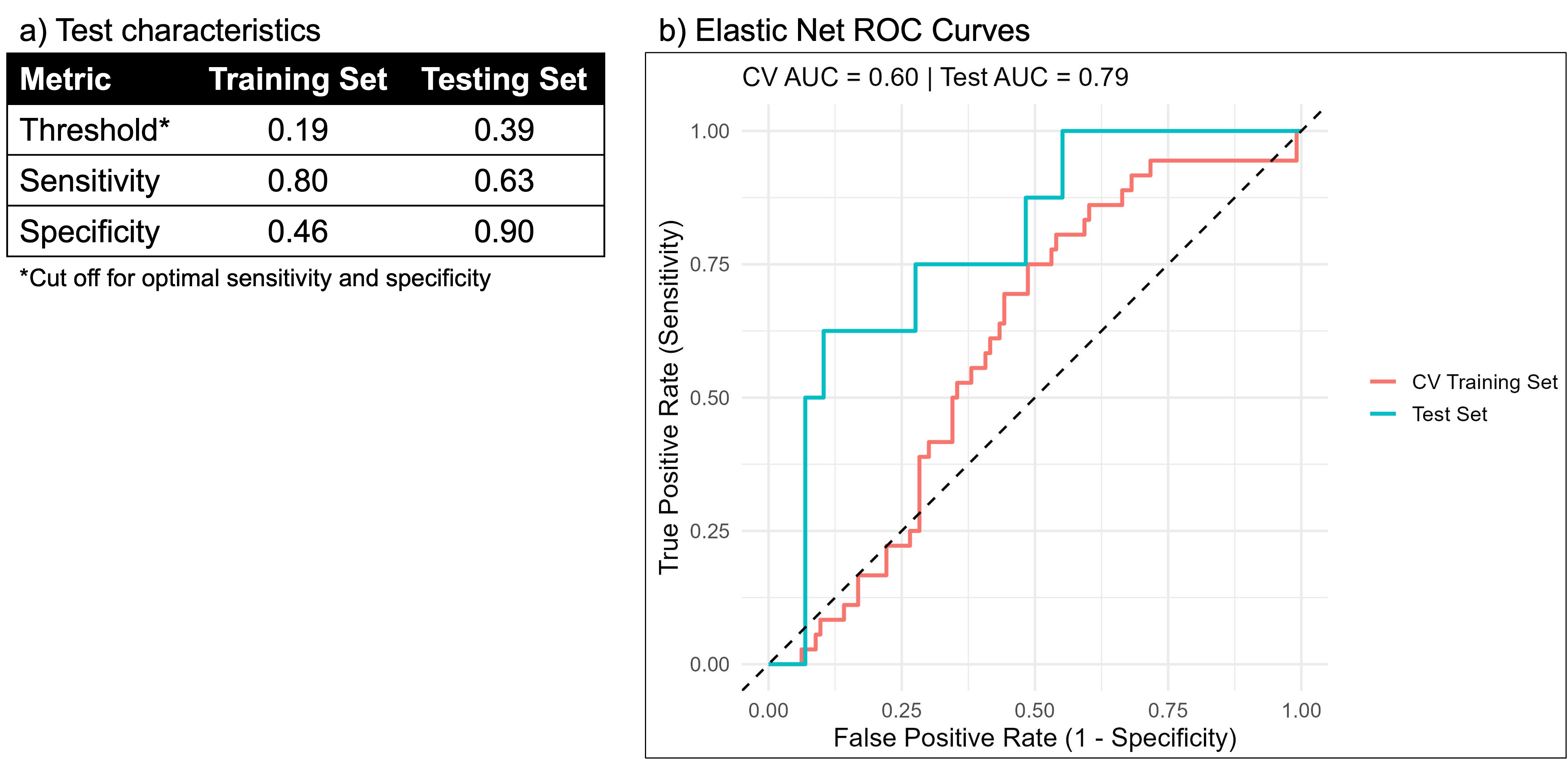
Background: Asthma exacerbations are a leading cause of pediatric emergency department (ED) visits and hospitalizations. Existing prediction tools rely on subjective clinical findings and do not reliably predict hospitalization early in the ED course. Respiratory impedance from oscillometry is a feasibly obtained objective lung function measure, which may be incorporated in prediction models to better assist clinicians with management and disposition decisions. Objective: To develop and internally validate a model that incorporates demographics, clinical factors and respiratory impedance metrics to predict hospitalization for children with asthma exacerbations in the ED. Design/Methods: Prospective study of children 4-18 years presenting to a pediatric ED for asthma exacerbations. Vital signs and respiratory impedance measures were obtained at ED presentation, prior to standard ED asthma therapies of inhaled bronchodilators and systemic corticosteroids. Demographics and asthma history were recorded. Respiratory impedance metrics include resistance (R-degree of airway obstruction) and reactance (X-degree of lung stiffness) over 10 frequencies 7-41Hz, frequency dependence of R (R7-19), area of X (AX) and resonant frequency (fres) transformed to z-scores from height-based reference equations. Data were split randomly into training (80%) and testing (20%) sets. The prediction model for hospitalization was developed and internally validated using elastic net regression with cross-validation to fine-tune the penalty terms. Youden's J-statistic was used to determine optimal sensitivity and specificity. Results: Of 186 participants (median age 9 years [IQR 6.6, 12.4]), 107 (58%) were male, 110 (59%) identified as Hispanic and 44 (24%) required hospitalization (Table includes all candidate variables). A combination of race, insurance type, initial vital signs (temperature, oxygen saturation, heart rate), and respiratory impedance measures (R19, R7-19, AX7, Fres) were retained in the final model and best differentiated hospitalization (AUC 0.79; 95% CI 0.62-0.96) with optimal testing set sensitivity of 0.63 and specificity of 0.90 (Figure).
Conclusion(s): Our internally validated model to predict hospitalization at initial ED presentation for asthma exacerbations includes objective physiologic measures that are feasible to obtain in this setting. Once externally validated, this prediction model may facilitate prompt management and disposition decisions for pediatric asthma exacerbations in the ED.
Table. Demographics, clinical characteristics, and respiratory impedance measures of study population included as candidate variables in elastic net models.
Figure. Optimal test characteristics in training and test sets (a) and elastic net ROC curves for cross-validated (CV) training set and test set (b) for outcome of hospitalization.

.jpeg.jpg "Melisa Tanverdi, MD (she/her/hers) photo")