Session: Infectious Diseases 2: Antimicrobial and Diagnostic Stewardship
410 - Clinician Knowledge, Attitudes, and Practices on Procalcitonin (PCT) in a Pediatric Health System
Saturday, April 25, 2026
3:30pm - 5:45pm ET
Publication Number: 2398.410
Charmaine P. Mutucumarana, Children's Hospital of Philadelphia, Philadelphia, PA, United States; Kathleen Chiotos, Children's Hospital of Philadelphia, Philadelphia, PA, United States; Anyun Chatterjee, Children's Hospital of Philadelphia, Philadelphia, PA, United States; Katherine S. Kellom, Children's Hospital of Philadelphia, Philadelphia, PA, United States; Tracey Polsky, Perelman School of Medicine at the University of Pennsylvania, Philadelphia, PA, United States; Laura Sartori, Childrens Hospital of Philadelphia, Philadelphia, PA, United States; Joseph J. Zorc, Childrens Hospital of Philadelphia, Wynnewood, PA, United States; Rebecca Same, Childrens Hospital of Philadelphia, Philadelphia, PA, United States
Fellow Physician Children's Hospital of Philadelphia Philadelphia, Pennsylvania, United States
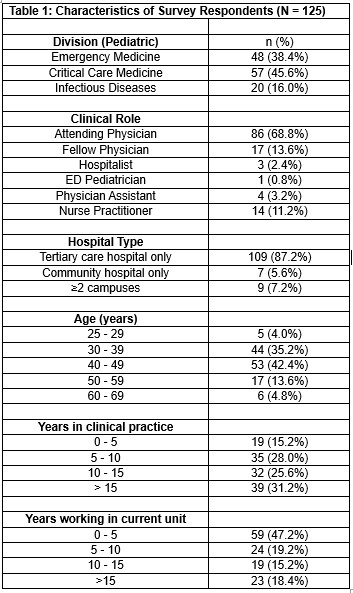
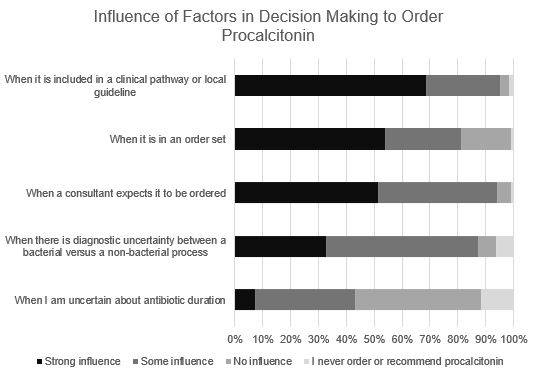
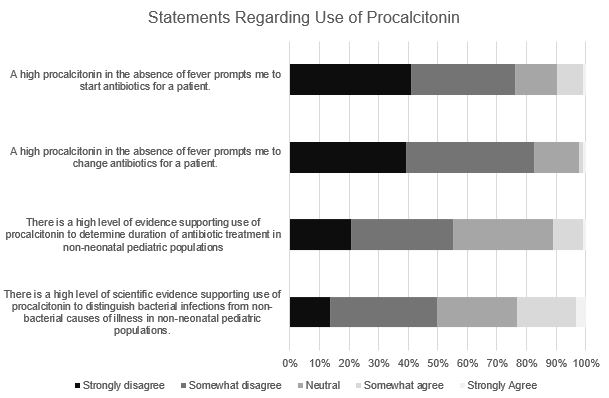
Background: Procalcitonin (PCT) is a commonly ordered inflammatory marker, but validated uses in children are limited. Pediatric clinicians' knowledge, attitudes, and practices regarding PCT are poorly understood. Objective: To evaluate pediatric clinicians' use of PCT, knowledge of the evidence regarding its use in children, and contextual factors influencing ordering practices. Design/Methods: We performed a single-center observational study to quantify PCT orders by specialty at Children's Hospital of Philadelphia (CHOP) from October 2024 to September 2025. We then used an electronic survey to measure knowledge, attitudes, and practices about PCT use among Emergency Department (ED), Pediatric Intensive Care Unit (PICU), and Infectious Diseases (ID) attendings, fellows, hospitalists, nurse practitioners, and physician assistants at CHOP. The survey presented clinical vignettes of patients with varied clinical severity to assess likelihood of ordering a PCT ("Yes/No") and confidence in this decision (assessed on Likert scale). We also assessed knowledge of the evidence supporting PCT use in children, and factors influencing PCT ordering. Clinicians who reported ordering PCT in ≤1 vignette were considered low PCT users, while those who would order it in 2 or more were considered high users. Demographics of respondents were collected. Results: During the one-year study period, 4966 PCT tests were performed, 37% in the ED and 26% in the PICU. There were 125 survey respondents, with attending physicians accounting for 69% (Table 1). Of 48 ED and 57 PICU clinicians, 40% and 32% were high utilizers of PCT (p = 0.39). All ID clinicians were low PCT utilizers. A recommendation for PCT in a clinical pathway or order set was reported to have the strongest influence on ordering; however, 68% of PCT were ordered outside of order sets (Figure 1). Diagnostic uncertainty between a bacterial and non-bacterial process influence PCT ordering, but 41% reported not using a specific cutoff value. Among those who did, the median threshold for bacterial infection was 1 ng/mL (IQR 0.5-3). A minority of clinicians (23%) agreed that strong evidence supports PCT for distinguishing bacterial from non-bacterial illness in non-neonatal pediatric populations (Figure 2). Sixty percent perceived institutional ordering of PCT as excessive.
Conclusion(s): Reported PCT use among clinicians varies across specialties and there are discrepancies between reported and actual practice. We are exploring these findings with qualitative research to better understand clinician decision-making and help standardize evidence-based utilization of PCT in pediatrics.
Table 1: Characteristics of Survey Respondents (N = 125)
Figure 1: Influence of Factors in Decision Making to Order Procalcitonin
Figure 2: Level of Agreement with Statements Regarding Use of Procalcitonin

.jpg "Charmaine P. Mutucumarana, MD (she/her/hers) photo")