577 - Fourteen-Year Trends in Pediatric Empyema Admissions, Management, and Outcomes in a Tertiary Care Pediatric Hospital
Saturday, April 25, 2026
3:30pm - 5:45pm ET
Publication Number: 2562.577
Johan Bouwer, University of British Columbia Faculty of Medicine, Vancouver, BC, Canada; Siyabulela N. Bovula, BC Children's Hospital, Vancouver, BC, Canada; Jeffrey Bone, BCCHR, Vancouver, BC, Canada; Sameena Somani, University of British Columbia, Vancouver, BC, Canada; Claire Seaton, BC Children's Hospital, Vancouver, BC, Canada; Manish Sadarangani, University of British Columbia Faculty of Medicine, Vancouver, BC, Canada; Nassr Nama, Seattle Children's Hospital, Seattle, WA, United States; Clara Fernandez Elviro, Chuv, Lausanne, Vaud, Switzerland; Connie Yang, The Hospital for Sick Children, Toronto, ON, Canada
Medical Student University of British Columbia Faculty of Medicine Vancouver, British Columbia, Canada
Background: Community-acquired pneumonia with effusion or empyema remains a significant cause of pediatric hospitalization. Objective: Describe the epidemiology, management, and outcomes of pediatric community-acquired pneumonia with effusion at the sole tertiary pediatric hospital in British Columbia, Canada. Design/Methods: Patients admitted to BC Children's Hospital between January 1, 2020 and April 30, 2024 with pneumonia and pleural effusion were identified from the discharge abstract database (ICD10 code J86 or J86.9 or J90+J12, J13, J14, J15 or J18). Charts manually reviewed to confirm eligibility (inclusion: 0 to 18 years of age, admitted with infectious history and pneumonia with more than a trivial effusion, exclusion: chest tube or surgical management prior to transfer, fungal or mycobacterial cause, significant comorbidity), and to collect clinical data. Results: 259 patients included with a median age 5.5 years [IQR 3.2-7.6], 48.3% were female. The majority (n=150, 57.9%) were transferred from another hospital where they had received IV antibiotics. 63% of patients had a bacterial pathogen found: Streptococcus pneumoniae (40%), Streptococcus pyogenes (13%), Mycoplasma pneumoniae (6%) and Staphylococcus aureus (2%). 33% had positive viral testing: rhinovirus/enterovirus (12%), human metapneumovirus (9%), influenza (6%).
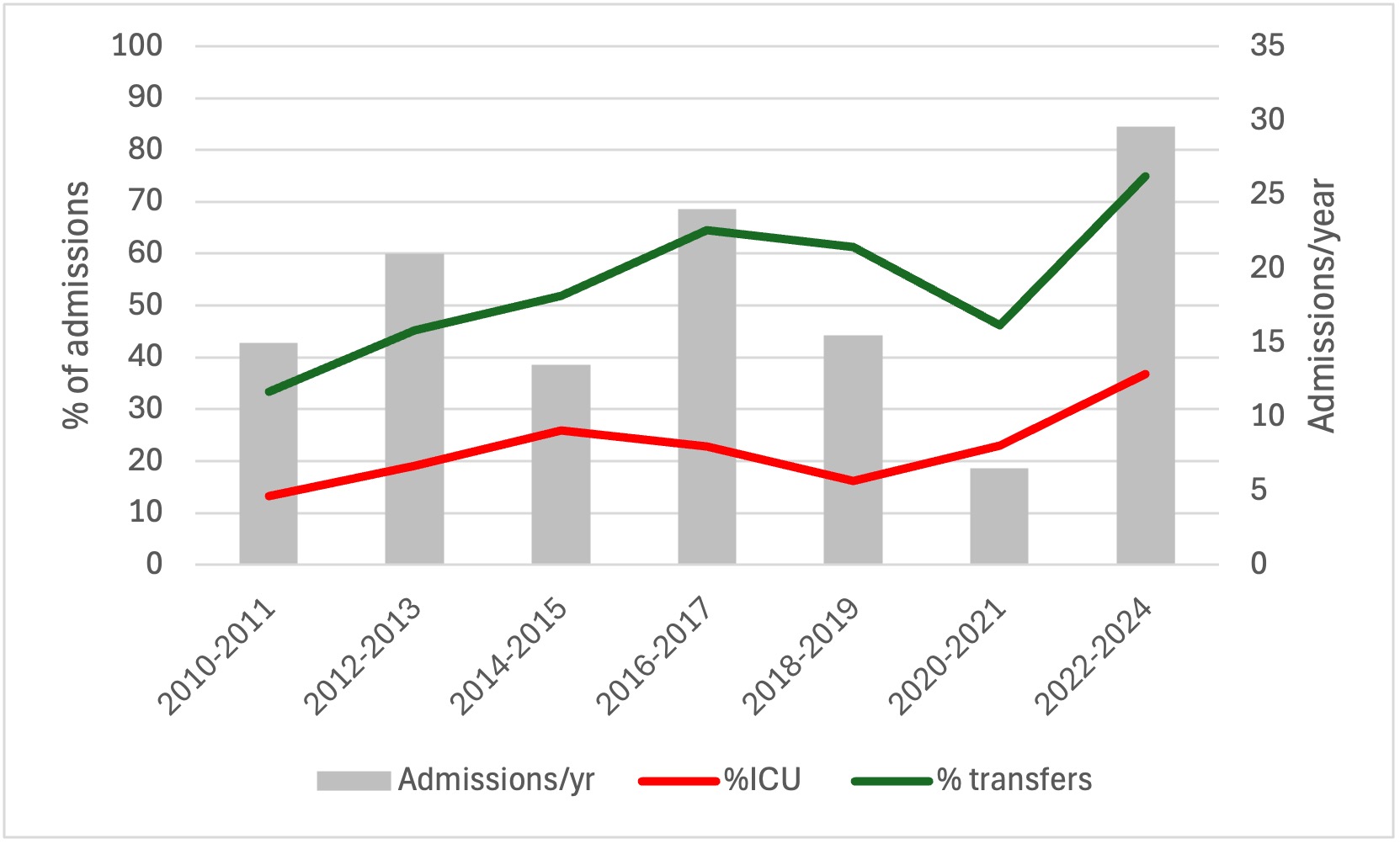
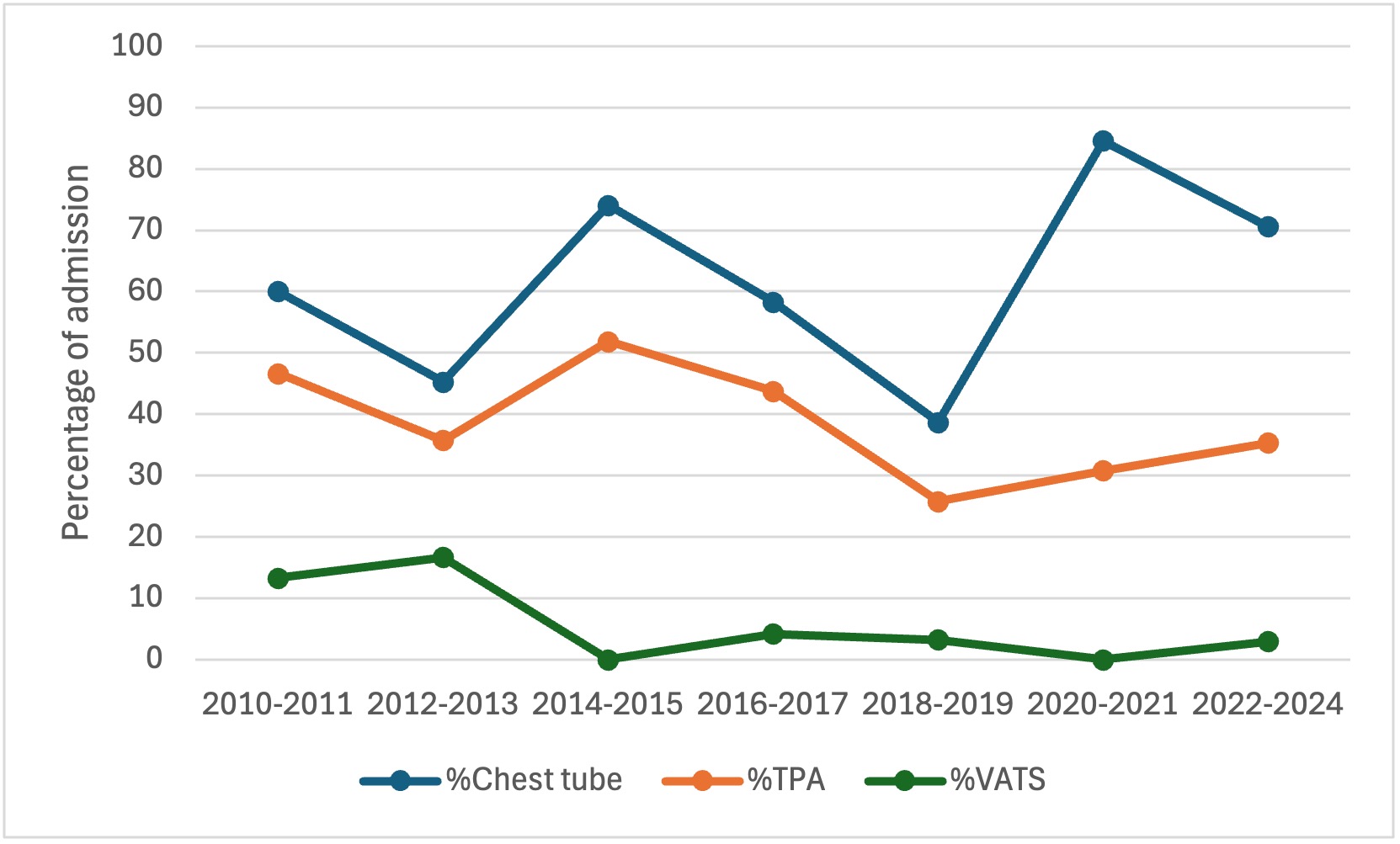
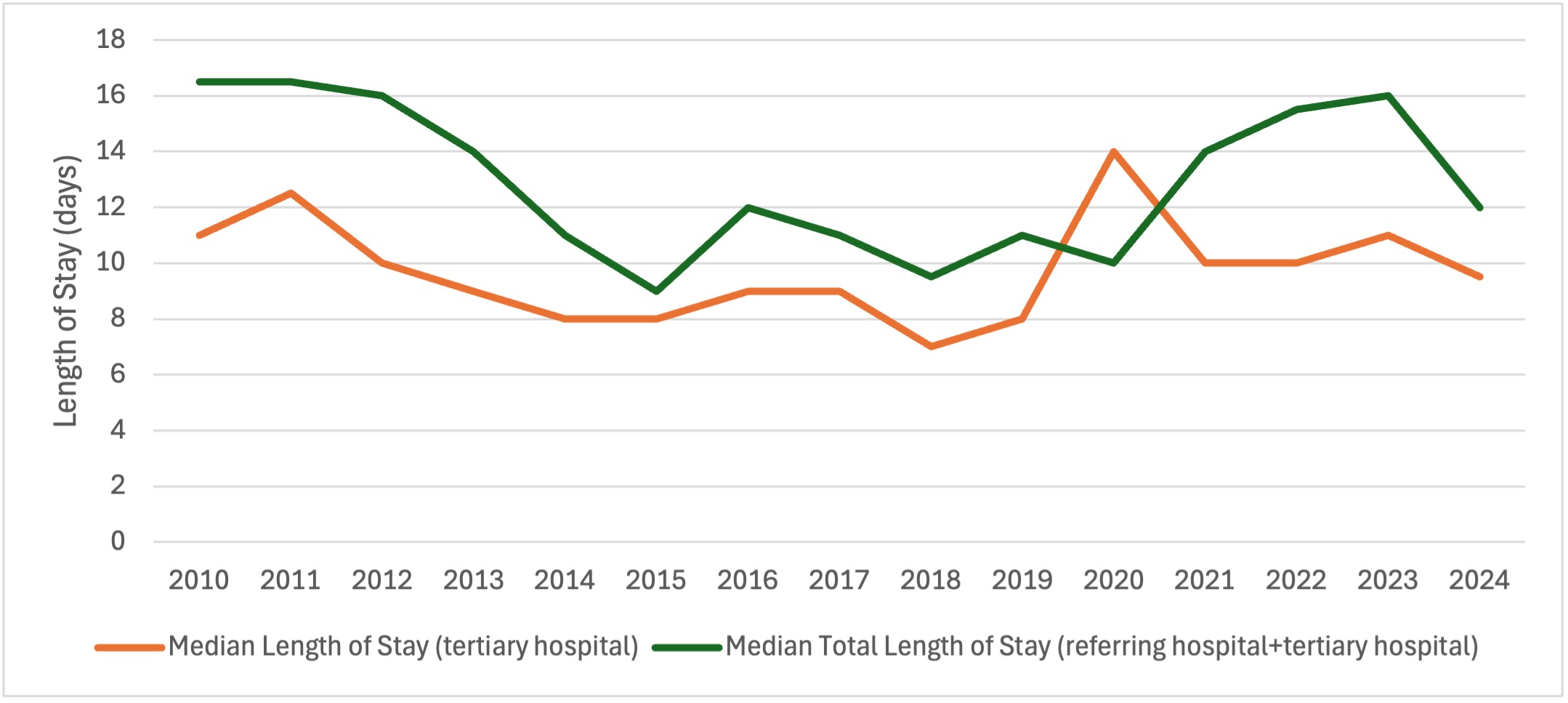
From 2010 to 2024, admissions were 7 to 30/year with a nadir in 2020-2021(Fig 1). Overall, there was an increasing trend in patients transferred from other hospitals and intensive care unit (ICU) admission, (24%, n =63). (Fig 1). There was significant variability in % of patients receiving chest tubes with or without TPA, and rates of Video-Assisted Thoracostomy Surgery (VATS) was low. (Fig 2). Median length of stay (LOS) at tertiary care hospital was 9 days (IQR 7-14) and median total LOS (includes days at referring hospital) was 12 days (IQR 9-16) (Fig 3). There were no deaths.
Conclusion(s): We found no mortality but high inpatient resource use: 60% of patients transferred from other hospitals, 24% requiring ICU, and median LOS of 9 days. LOS has not significantly changed over time in patients largely treated with antibiotics or chest tubes and is similar to other studies, including those with primary surgical management.
Next phase of the study will include a cohort from Seattle Children's Hospital to compare management strategies and outcomes, and to assess whether primary treatment with a chest tube is associated with a decreased length of stay compared to antibiotics alone.
Figure 1: Hospital, ICU admissions and transfers from other hospitals from 2010 to 2024
Figure 2: Empyema management strategies from 2010 to 2024
Figure 3: Median length of stay for pediatric empyema from 2010 to 2024

 photo")