565 - Nitrous Oxide vs Ketamine: Impacts on Pediatric Emergency Department Length of Stay
Saturday, April 25, 2026
3:30pm - 5:45pm ET
Publication Number: 2550.565
Tabitha V. Brock, Medical City Children's Hospital, Dallas, TX, United States; Anna Suessman, Medical City Children's Hospital, Dallas, TX, United States
Pediatric System Advanced Practice Provider Director Medical City Children's Hospital Dallas, Texas, United States
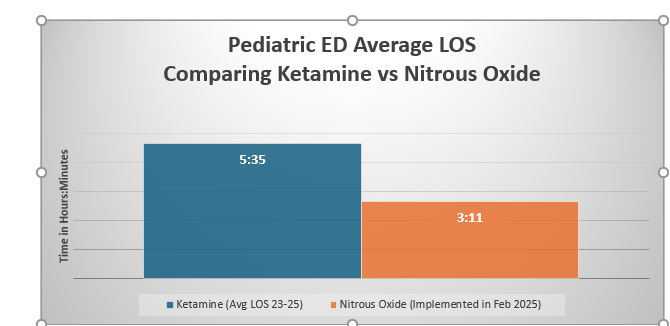
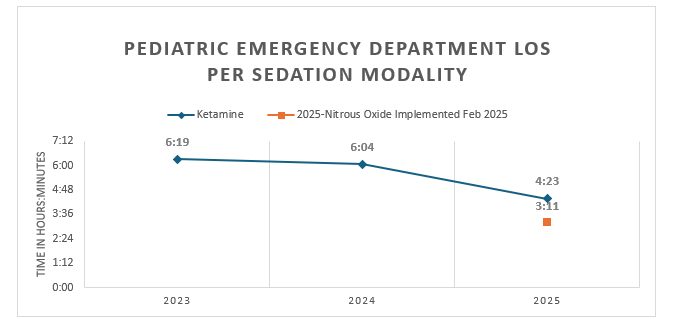
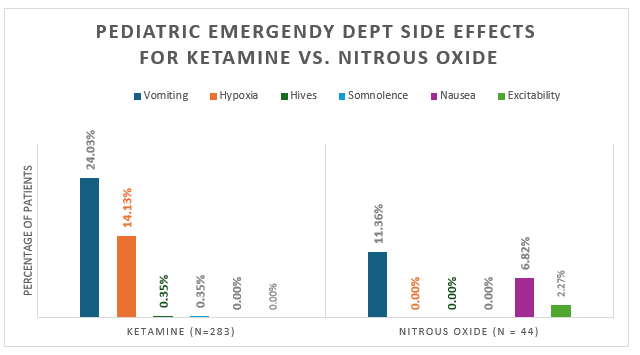
Background: Nitrous oxide (N₂O) is a well-established analgesic and anxiolytic agent, widely used for procedural sedation in pediatric dentistry. Despite its demonstrated safety and efficacy, its use in Pediatric Emergency Departments (PEDs) remains limited and underexplored. To address this gap, we implemented a comprehensive training program for PED providers and introduced N₂O as an alternative sedation agent. We hypothesized that using N₂O for procedural sedation would significantly reduce patient length of stay (LOS) without compromising safety or outcomes. Objective: We hypothesized that using N2) for procedural sedation would significantly reduce patient LOS without compromising safety or outcomes. Design/Methods: We conducted a retrospective chart review of pediatric patients who underwent painful procedures in a tertiary children's hospital emergency department. The study was reviewed and approved by the hospital's Institutional Review Board (IRB). The primary outcome was LOS in patients receiving ketamine versus N₂O. Secondary outcomes included procedure type and complications. Data for ketamine were collected from January 1, 2023, to December 31, 2024, and for N₂O from March 1, 2025 (inception) to August 31, 2025. De-identified data were analyzed to compare LOS between the two sedation modalities using inferential statistics (independent samples t-test); side effects were descriptively summarized. Results: Out of 288 patients who received ketamine sedation, 260 met inclusion criteria, with a mean LOS of 459.40 minutes (Sd, 166). In comparison, 47 patients who received nitrous oxide (N₂O), 43 of whom met inclusion criteria, with a mean LOS of 190.95 (sd, 81.43) minutes. With a mean difference of 268 minutes (Welch's t (111.1)=16.6, p < .001) and a large effect size (Cohen's d = 1.71), this finding reflects a clinically and operationally meaningful reduction in LOS with N₂O. Data collection for N₂O is ongoing to complete a one-year comparison between the two agents.
Conclusion(s): Nitrous oxide is a safe and effective procedural sedation option that significantly reduced LOS and is associated with fewer adverse events compared to ketamine. Implementing nitrous oxide as an alternative to ketamine enhances pediatric procedural care by significantly shortening LOS by over 4 hours, potentially reducing emergency department crowding and resource utilization while improving the patient experience.

 photo")