489 - Antibody-Mediated Rejection Outcomes of Pediatric Renal Transplants with Strict HLA-DR/DQ Epitope Matching
Saturday, April 25, 2026
3:30pm - 5:45pm ET
Publication Number: 2476.489
Dinah Batchelor, University of Tennessee Health Science Center College of Medicine, Memphis, TN, United States; Ethan G. Lilly, Le Bonheur Children's Hospital, Brentwood, TN, United States; Sallyanne C. Fossey, DCI Inc., Nashville, TN, United States; Bradley Hyman, University of Tennessee Health Science Center College of Medicine, Memphis, TN, United States; Marygrace Duggar, St. Jude Children's Research Hospital, Memphis, TN, United States; Rima Zahr, University of Tennessee Health Science Center College of Medicine, Memphis, TN, United States
Pediatric Nephrology Fellow University of Tennessee Health Science Center College of Medicine Memphis, Tennessee, United States
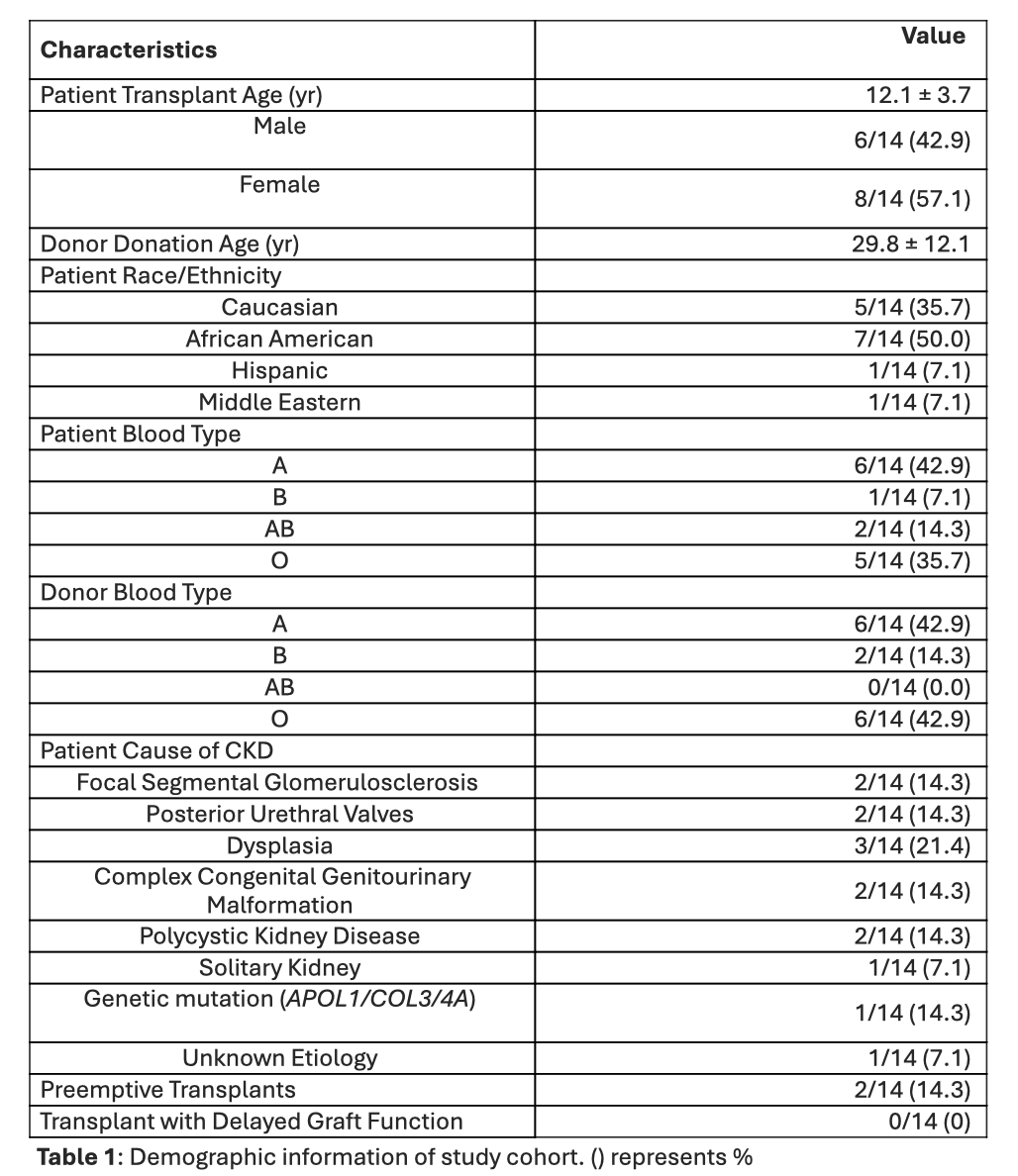
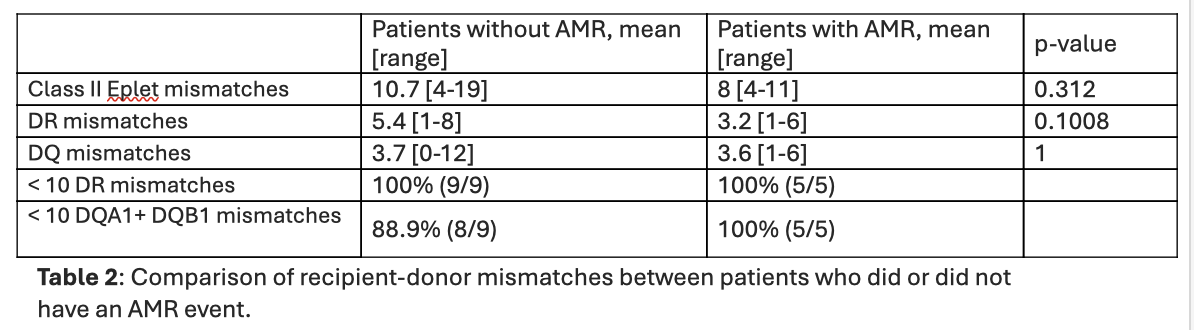
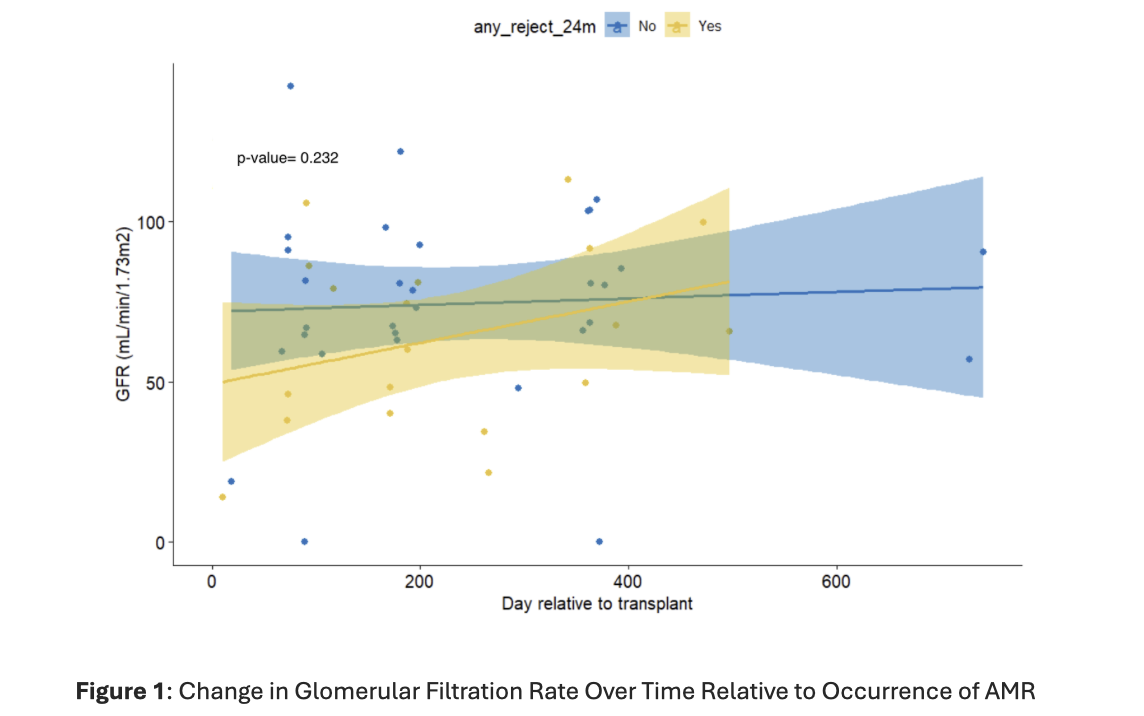
Background: Pediatric renal allograft rejection and long-term outcomes remain under investigation. Recent advances have highlighted the utility of non-invasive methods for identifying predictors of adverse outcomes. Traditional human leukocyte antigen (HLA) matching of the HLA-A, -B, and -DR loci is associated with a reduced incidence of de novo donor-specific antibodies (DSAs) and subsequent graft rejection. Increased alloimmune risk has been linked to higher HLA class II epitope mismatch loads, particularly at the DQ and DR loci. Improved HLA class II matching may enable individualized risk stratification and tailoring of immunosuppression. Objective: To describe antibody-mediated rejection (AMR) outcomes in pediatric kidney transplant recipients strictly matched at DQ and DR HLA epitopes. Design/Methods: This IRB-approved, single-center retrospective cohort study included 14 pediatric kidney transplant recipients from January 2023-December 2024. Donor-recipient pairs had ≤10 epitope mismatches at each of the DR and DQ loci. AMR was confirmed by biopsy, and treatment included steroid pulse, intravenous immunoglobulin, Rituximab, and ± plasmapheresis. Characteristics of patients were described by mean and range for continuous variables, and frequency and percentage of categorical variables. Comparison between non-AMR and AMR groups was performed by permutation testing (significance: p< 0.05). Kidney function over time relative to occurrence of AMR was analyzed using Spearman regression and one-way ANOVA. Results: In our cohort, the mean age was 12.1 years, 57% female, and predominantly had kidney failure due to congenital anomalies (57%). AMR occurred in 5/14 (35.7%) patients, with a mean time of occurrence at 8 months post-transplant, mostly within the first year (4/5, 80%). DSA profiles varied: one patient had 2 class I DSAs at < 3 months; another had 2 class I and 1 class II at 4-6 months; two patients averaged 2.5 DSAs at 7-12 months; one had 1 class II DSA at 12-24 months. AMR patients were more strictly matched at DR/DQ epitopes, mean of 8 vs 10.7 class II mismatches, but this was not statistically significant (p-value = 0.312). The change in glomerular filtration rate over time relative to occurrence of AMR was also not statistically significant (p-value 0.232).
Conclusion(s): Despite strict epitope matching, 35% of patients developed de novo class II AMR. No significant difference in kidney function was observed between AMR and non-AMR groups at the last follow up. Future direction will assess antibody resolution and continued prospective monitoring.
Demographic information of study cohort
Comparison of recipient-donor mismatches between patients who did or did not have an AMR event.
Change in Glomerular Filtration Rate Over Time Relative to Occurrence of AMR

 photo")